The procedure of filling out the lab form 183 is actually hassle-free. We made certain our editor is easy to understand and can help fill out almost any document without delay. Below are a couple of steps you will have to follow:
Step 1: First of all, click on the orange "Get form now" button.
Step 2: Now you are on the form editing page. You can change and add text to the file, highlight specified content, cross or check specific words, include images, put a signature on it, get rid of needless fields, or eliminate them altogether.
The following parts are what you are going to fill out to obtain the finished PDF document.
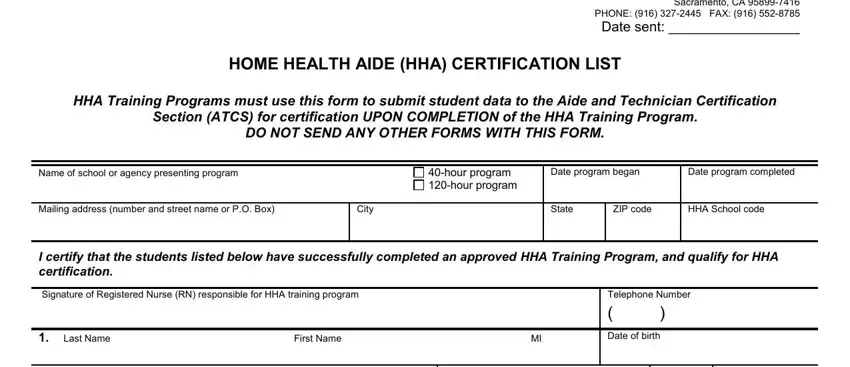
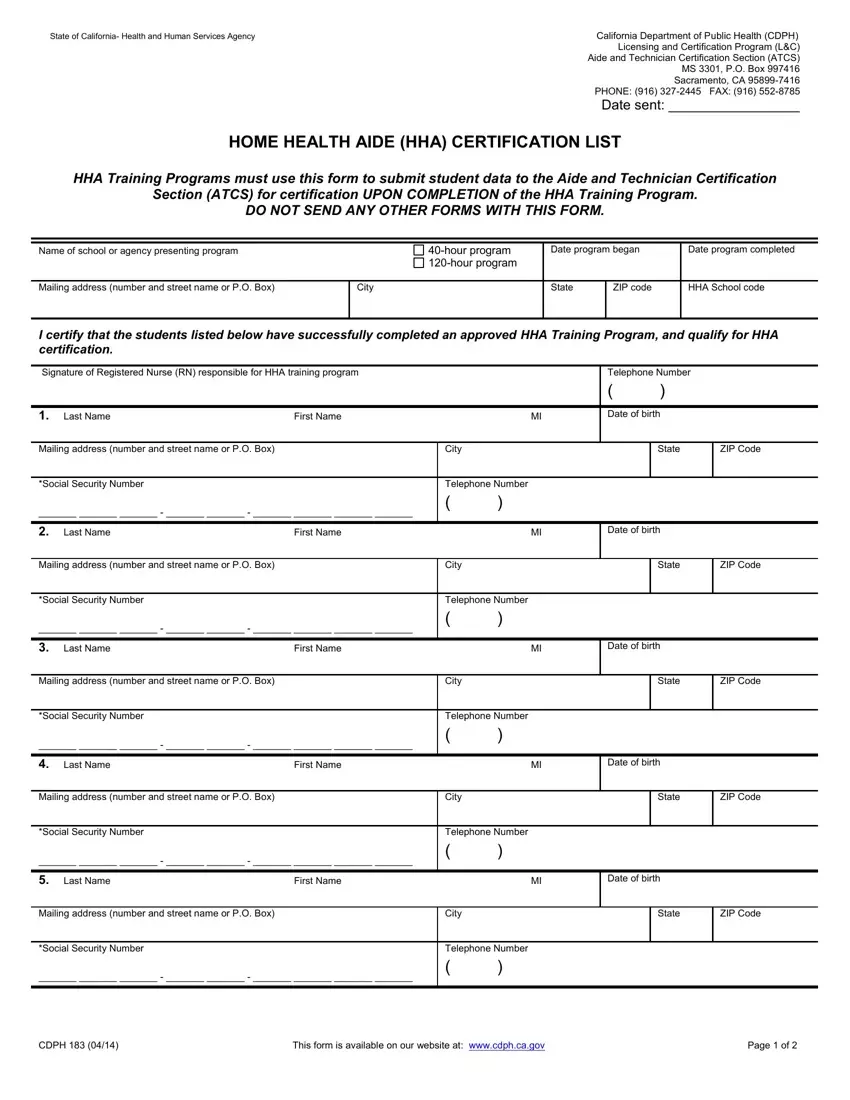
Provide the asked particulars in the Mailing address number and street, City, State, ZIP Code, Social Security Number, Telephone Number, Last Name First Name MI Date of, Mailing address number and street, City, State, ZIP Code, Social Security Number, Telephone Number, Last Name First Name MI Date of, and Mailing address number and street area.
The application will require data to quickly fill out the part Mailing address number and street, City, State, ZIP Code, Social Security Number, Telephone Number, CDPH, and This form is available on our.
The Last Name First Name MI Date of, Mailing address number and street, City, State, ZIP Code, Social Security Number, Telephone Number, Last Name First Name MI Date of, Mailing address number and street, City, State, ZIP Code, Social Security Number, Telephone Number, and Last Name First Name MI Date of area allows you to point out the rights and responsibilities of both sides.
Finish by analyzing the following areas and submitting the appropriate details: Last Name First Name MI Date of, Mailing address number and street, City, State, ZIP Code, Social Security Number, Telephone Number, Last Name First Name MI Date of, Mailing address number and street, City, State, ZIP Code, Social Security Number, Telephone Number, and Last Name First Name MI Date of.
Step 3: Hit the Done button to save the file. Then it is readily available for transfer to your gadget.
Step 4: To prevent yourself from probable upcoming complications, take the time to obtain at the very least two or three copies of each and every document.
