The rhb permits filling in course of action is very simple. Our PDF tool lets you work with any PDF file.
Step 1: Choose the orange button "Get Form Here" on this webpage.
Step 2: The document editing page is right now available. You can add information or update current information.
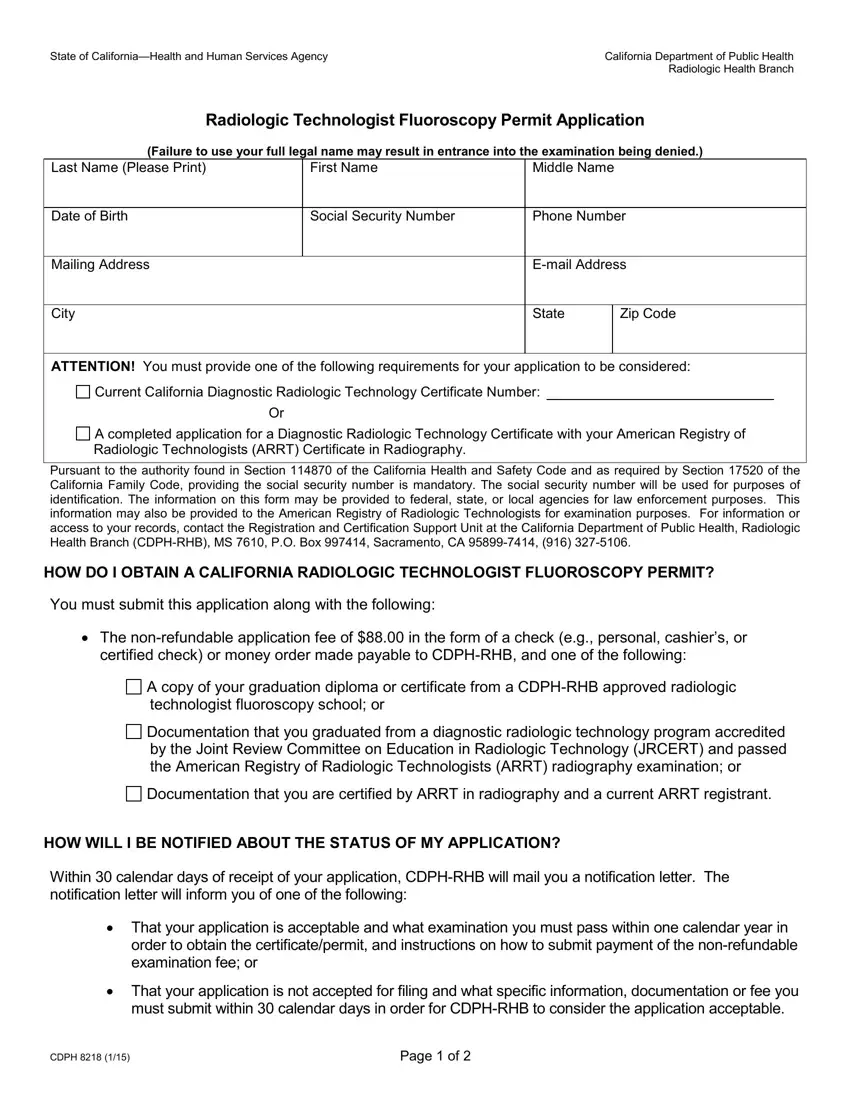
Provide the necessary details in every segment to fill in the PDF rhb permits
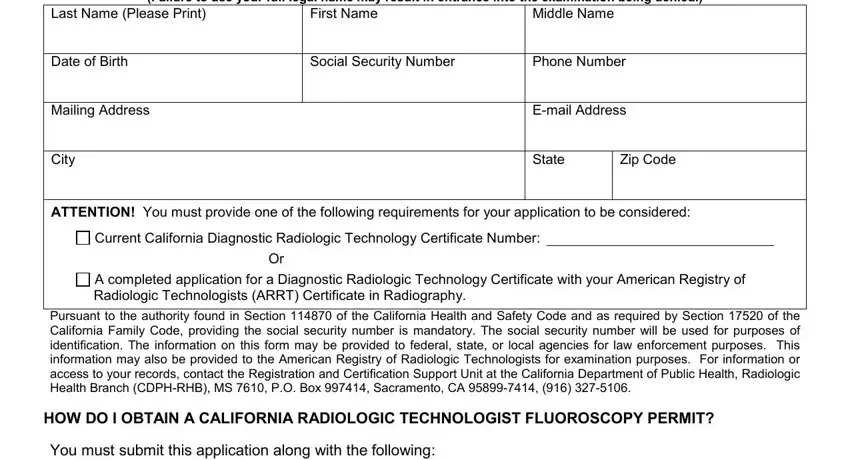
In the certified check or money order, A copy of your graduation diploma, Documentation that you graduated, Documentation that you are, HOW WILL I BE NOTIFIED ABOUT THE, Within calendar days of receipt, That your application is, order to obtain the, and That your application is not area, write down your details.
Within the segment referring to Last Name Please Print, First Name, Middle Name, HOW DO I SUBMIT MY APPLICATION, Please mail this application all, California Department of Public, and I certify that the information, you should note some essential details.
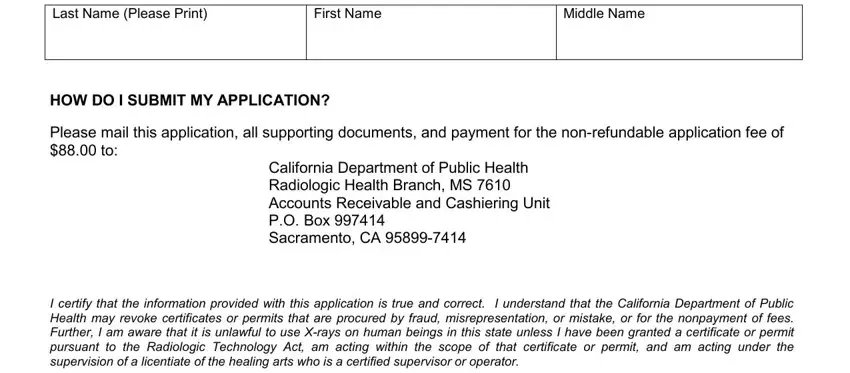
You'll need to describe the rights and obligations of both sides in space Signature, and Date.
Step 3: Click the Done button to save your form. Then it is ready for upload to your device.
Step 4: Create a duplicate of each file. It would save you some time and make it easier to stay clear of problems down the road. Also, your data isn't revealed or monitored by us.
