
You could fill in 932 form instantly with the help of our online PDF tool. In order to make our editor better and less complicated to work with, we continuously develop new features, considering feedback coming from our users. Starting is effortless! Everything you should do is follow the following easy steps directly below:
Step 1: Access the PDF doc in our editor by pressing the "Get Form Button" at the top of this webpage.
Step 2: With our handy PDF editing tool, you are able to do more than merely fill in forms. Try all the features and make your documents look perfect with custom textual content added in, or modify the original content to perfection - all that supported by an ability to insert stunning graphics and sign the file off.
It will be straightforward to finish the pdf using out practical tutorial! Here is what you should do:
1. The 932 form involves certain details to be entered. Make sure the subsequent fields are completed:
2. Your next step is to fill in the next few blank fields: I certify under penalty of the, APPLICANTS SIGNATURE, DATE, APPLICANTS DO NOT USE THE SPACE, CASH, NHAP INITIALS, AMOUNT, CDPH, STATUS, Approved, Rejected, Denied, Missing Information, Correct Fees, and State Certification.
It's very easy to make a mistake while completing the Rejected, and so ensure that you go through it again before you decide to send it in.
3. Completing APPLICANTS NAME Last, First, SOCIAL SECURITY NUMBER, Are you now or have your ever, Yes, below, Agency Agency Agency, License License License, Date of expiration Date of, Have you ever pled guilty or nolo, Yes, IF THE ANSWER TO THIS QUESTION IS, Have you ever allowed your NHA, Yes, and If Yes identify the State Agency is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
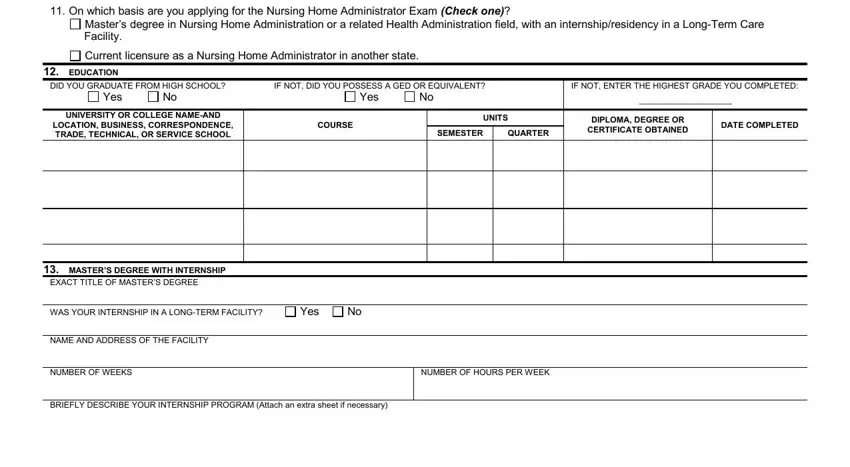
4. Filling in On which basis are you applying, Masters degree in Nursing Home, Current licensure as a Nursing, EDUCATION, DID YOU GRADUATE FROM HIGH SCHOOL, IF NOT DID YOU POSSESS A GED OR, IF NOT ENTER THE HIGHEST GRADE YOU, Yes, Yes, UNIVERSITY OR COLLEGE NAMEAND, LOCATION BUSINESS CORRESPONDENCE, COURSE, UNITS, SEMESTER, and QUARTER is essential in this next stage - don't forget to take the time and take a close look at each field!
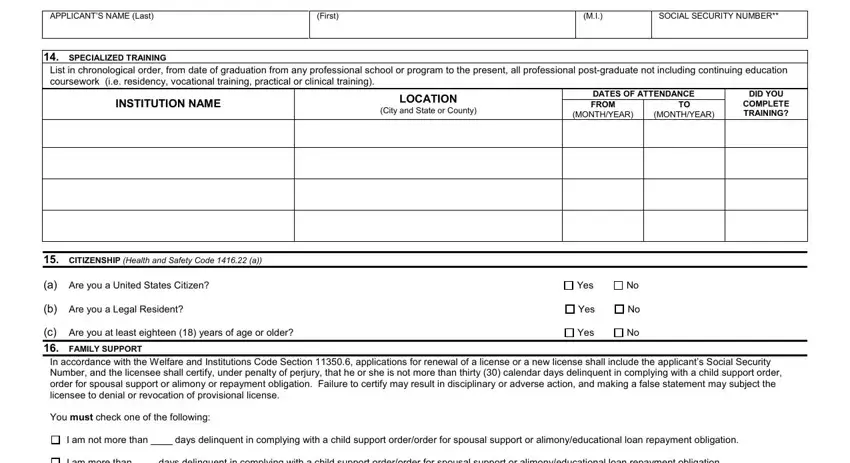
5. Last of all, this last section is what you will need to complete prior to closing the form. The fields in this case are the following: APPLICANTS NAME Last, First, SOCIAL SECURITY NUMBER, SPECIALIZED TRAINING, List in chronological order from, INSTITUTION NAME, LOCATION, City and State or County, DATES OF ATTENDANCE FROM, MONTHYEAR, MONTHYEAR, DID YOU, COMPLETE TRAINING, CITIZENSHIP Health and Safety, and a Are you a United States Citizen.
Step 3: Right after taking another look at the fields and details, hit "Done" and you're good to go! Go for a 7-day free trial plan at FormsPal and get immediate access to 932 form - downloadable, emailable, and editable from your FormsPal account page. Here at FormsPal.com, we endeavor to make certain that all of your details are maintained protected.