
E-mail can be completed online effortlessly. Just use FormsPal PDF editing tool to complete the task in a timely fashion. In order to make our editor better and more convenient to work with, we continuously design new features, taking into account feedback from our users. In case you are looking to get going, this is what it's going to take:
Step 1: Access the PDF in our editor by pressing the "Get Form Button" above on this page.
Step 2: Using our advanced PDF tool, you could do more than simply complete blank fields. Try all of the functions and make your forms seem perfect with customized textual content put in, or modify the original content to perfection - all that accompanied by an ability to incorporate your own images and sign the document off.
This form will need specific details; in order to guarantee accuracy and reliability, please be sure to consider the subsequent recommendations:
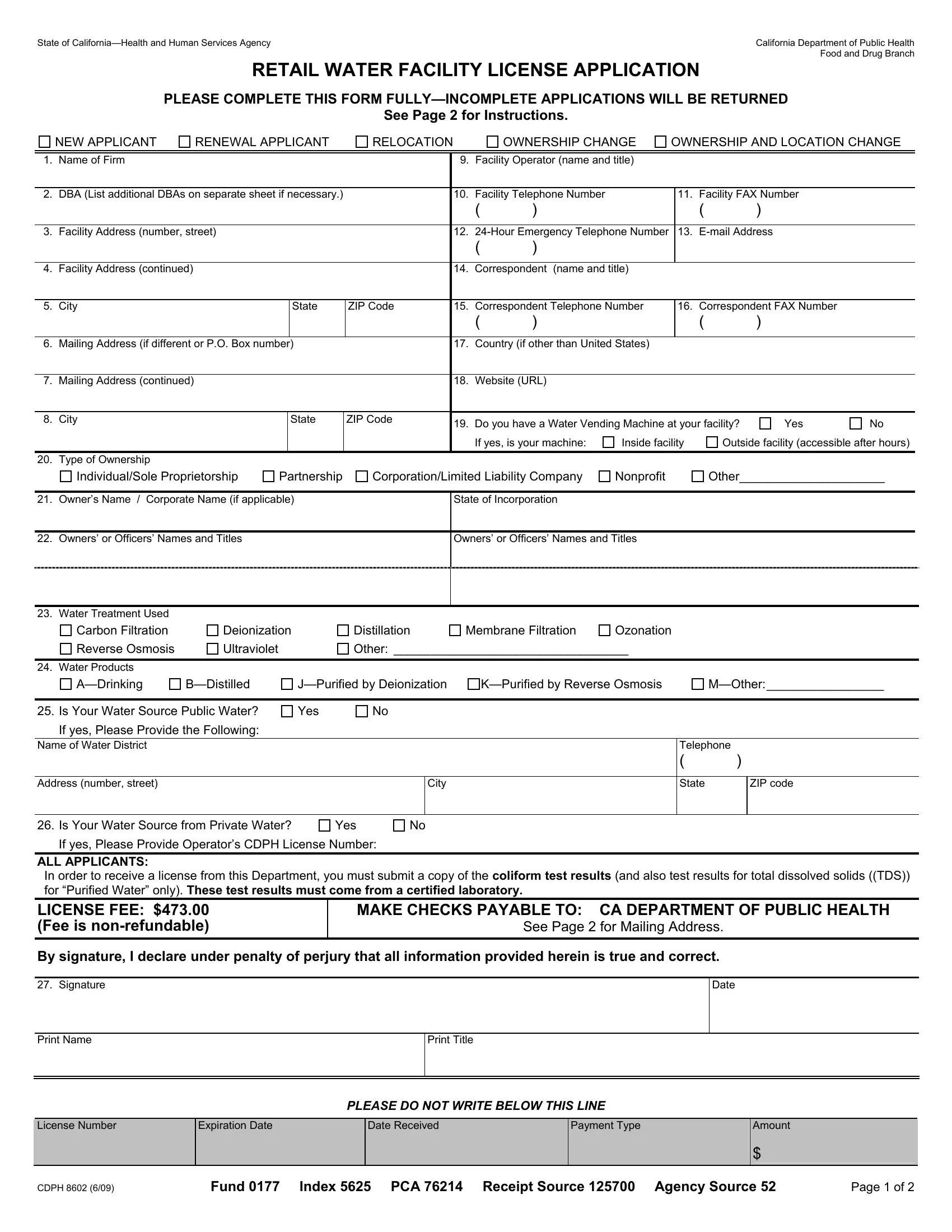
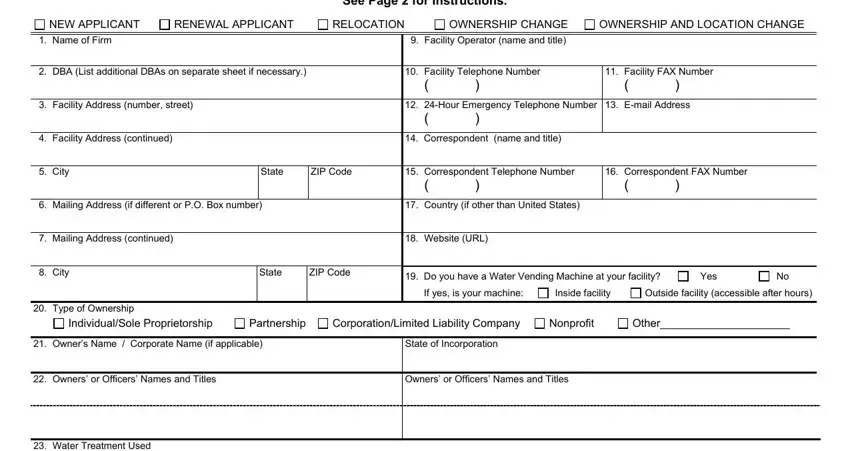
1. Whenever filling out the E-mail, be certain to incorporate all needed blank fields in its associated area. It will help expedite the process, allowing for your details to be handled promptly and accurately.
2. Now that the last segment is complete, it's time to insert the required specifics in Water Treatment Used Carbon, Reverse Osmosis, Water Products, ADrinking, Deionization, Ultraviolet, Distillation, Membrane Filtration, Ozonation, Other, BDistilled, JPurified by Deionization, KPurified by Reverse Osmosis, MOther, and Is Your Water Source Public Water so you're able to proceed to the third step.
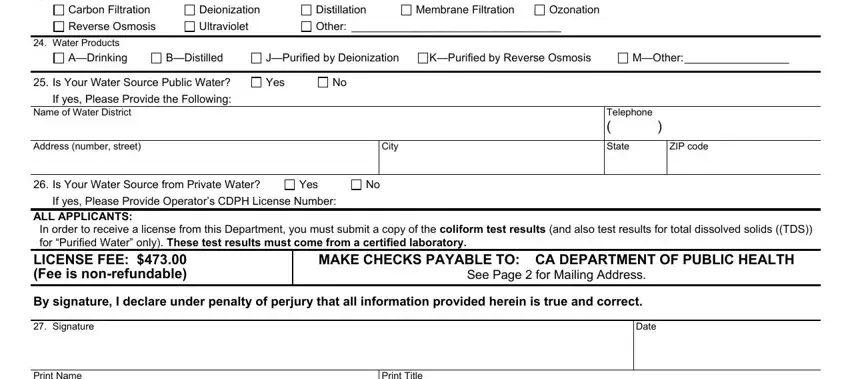
A lot of people generally get some points wrong when completing BDistilled in this part. Don't forget to revise what you type in here.
3. The next stage will be simple - fill out all the fields in Print Name, Print Title, License Number, Expiration Date, Date Received, Payment Type, PLEASE DO NOT WRITE BELOW THIS LINE, Amount, CDPH, Fund Index PCA Receipt Source, and Page of in order to finish the current step.

Step 3: Proofread all the details you've entered into the form fields and click on the "Done" button. Grab your E-mail the instant you join for a 7-day free trial. Instantly access the pdf in your FormsPal account, together with any modifications and changes being all synced! FormsPal guarantees secure form editor with no data recording or any type of sharing. Be assured that your details are secure with us!