State of California—Health and Human Services Agency |
California Department of Public Health |
|
Food and Drug Branch |
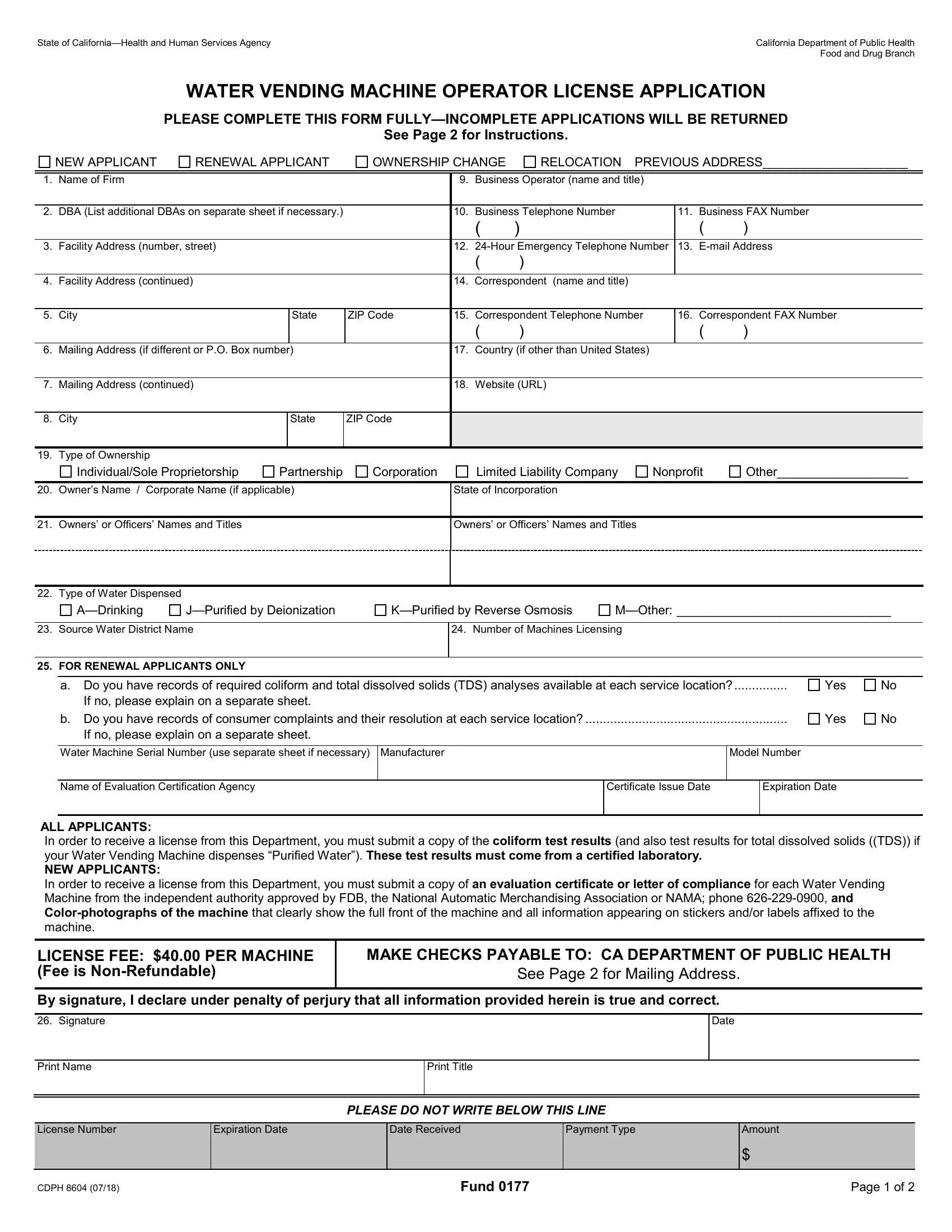
WATER VENDING MACHINE OPERATOR LICENSE APPLICATION
PLEASE COMPLETE THIS FORM FULLY—INCOMPLETE APPLICATIONS WILL BE RETURNED
See Page 2 for Instructions.
RELOCATION PREVIOUS ADDRESS_____________________
1. |
Name of Firm |
|
|
|
9. |
Business Operator (name and title) |
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
DBA (List additional DBAs on separate sheet if necessary.) |
|
10. |
Business Telephone Number |
|
11. |
Business FAX Number |
|
|
|
|
|
|
( |
) |
|
|
( |
) |
|
|
|
|
|
|
|
|
|
3. |
Facility Address (number, street) |
|
|
|
12. |
24-Hour Emergency Telephone Number |
13. |
E-mail Address |
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
Facility Address (continued) |
|
|
|
14. |
Correspondent (name and title) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
City |
|
State |
ZIP Code |
15. |
Correspondent Telephone Number |
|
16. |
Correspondent FAX Number |
|
|
|
|
|
|
( |
) |
|
|
( |
) |
|
|
|
|
|
|
|
|
|
|
6. |
Mailing Address (if different or P.O. Box number) |
|
17. |
Country (if other than United States) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7. |
Mailing Address (continued) |
|
|
|
18. |
Website (URL) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8. |
City |
|
State |
ZIP Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
19. |
Type of Ownership |
|
|
|
|
|
|
|
|
|
|
|
Individual/Sole Proprietorship |
Partnership |
Corporation |
|
Limited Liability Company |
Nonprofit |
Other___________________ |
|
|
|
|
|
|
|
|
20. |
Owner’s Name / Corporate Name (if applicable) |
|
State of Incorporation |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21. |
Owners’ or Officers’ Names and Titles |
|
|
|
Owners’ or Officers’ Names and Titles |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
22. |
Type of Water Dispensed |
|
|
|
|
|
|
|
|
|
|
J—Purified by Deionization
K—Purified by Reverse Osmosis
M—Other: _______________________________
23. Source Water District Name
24. Number of Machines Licensing
25. FOR RENEWAL APPLICANTS ONLY
a. Do you have records of required coliform and total dissolved solids (TDS) analyses available at each service location?...............
If no, please explain on a separate sheet.
b. Do you have records of consumer complaints and their resolution at each service location? .........................................................
If no, please explain on a separate sheet.
Water Machine Serial Number (use separate sheet if necessary)
Name of Evaluation Certification Agency
ALL APPLICANTS:
In order to receive a license from this Department, you must submit a copy of the coliform test results (and also test results for total dissolved solids ((TDS)) if your Water Vending Machine dispenses “Purified Water”). These test results must come from a certified laboratory.
NEW APPLICANTS:
In order to receive a license from this Department, you must submit a copy of an evaluation certificate or letter of compliance for each Water Vending Machine from the independent authority approved by FDB, the National Automatic Merchandising Association or NAMA; phone 626-229-0900, and Color-photographs of the machine that clearly show the full front of the machine and all information appearing on stickers and/or labels affixed to the machine.
LICENSE FEE: $40.00 PER MACHINE (Fee is Non-Refundable)
MAKE CHECKS PAYABLE TO: CA DEPARTMENT OF PUBLIC HEALTH
See Page 2 for Mailing Address.
By signature, I declare under penalty of perjury that all information provided herein is true and correct.
PLEASE DO NOT WRITE BELOW THIS LINE
CDPH 8604 (07/18) |
Fund 0177 |
Page 1 of 2 |
Water Vending Machine Operator License Application Instructions
Please Type or Print your Application.
New Applicant/Renewal Applicant: Place an (X) in the box next to New Applicant if your firm has not previously applied for a Water Vending Machine Operator License at this location while under the current ownership. Place an (X) in the box next to Renewal Applicant if your firm has already obtained a Water Vending Machine Operator License and you are renewing that license. If this firm has changed location or ownership, please submit a new application for licensure.
1.Name of Firm: Enter the full name of business, corporation, company, or organization applying for licensure.
2.DBA: Enter any other name(s) your company is doing business as.
3.–5. Facility Address: Enter the number, street, city, state, and ZIP code for this facility location.
6.–8. Mailing Address: Enter the full mailing address if different from the facility address.
9.Business Operator: Enter the full name of the person who manages the operations of your business and their title.
10.Business Telephone Number: Enter the daytime business telephone number for your business.
11.Business FAX Number: Enter your business FAX number.
12.24-Hour Emergency Telephone Number: Enter the telephone number to be called in the event of an emergency.
13.E-mail Address: Enter the facility e-mail address.
14.Correspondent: Enter the name of the person to contact for information regarding this application and their title.
15.Correspondent Telephone Number: Enter the daytime business telephone number of the contact person.
16.Correspondent FAX Number: Enter the daytime business FAX number of the contact person.
17.Country: Enter the country where your facility is located if outside of the United States.
18.Website: Enter the website address for your business if applicable.
19.Type of Ownership: Place an (X) in the box adjacent to the description of how your business is legally owned.
20.Corporate Name: Enter the corporate name if applicable. Enter the State of Incorporation if applicable.
21.Owners’ or Officers’ Names and Titles: List the business owners’ or officers’ names and titles.
22.Type of Water Dispensed: Place an (X) in the box adjacent to the types of water products you dispense.
23.Source Water District Name: Enter the name of the water district providing the source water for your machines.
24.Number of Machines Licensing: Enter the number of machines that you are licensing.
25.For Renewal Applicants Only: Answer yes or no to questions a. and b. by placing an (X) in the box adjacent to the correct answer. Enter the water machine serial number, machine manufacturer, machine model number, name of evaluation certification agency, certificate issue date, and certificate expiration date. Attach a separate sheet if additional space is needed.
26.Sign the application, enter date signed, and print your name and title.
**LICENSE FEES ARE NON-REFUNDABLE AND NON-TRANSFERABLE TO OTHER LOCATIONS OR ENTITIES
MAKE CHECKS PAYABLE TO: CA DEPARTMENT OF PUBLIC HEALTH
MAIL APPLICATION AND CHECK TO: |
|
Regular Mail: California Department of Public Health |
Overnight Mail: California Department of Public Health |
Food and Drug Branch - Cashier |
Food and Drug Branch - Cashier |
MS 7602 |
1500 Capitol Avenue, MS-7602 |
P.O. Box 997435 |
Sacramento, CA 95814 |
Sacramento, CA 95899-7435 |
|
Call the Food and Drug Branch at (916) 324-2170 if you have additional questions about this application or the required attachments.
CDPH 8604 (07/18) |
Fund 0177 |
Page 2 of 2 |