
Our PDF editor makes it simple to complete documents. You don't need to undertake much to manage CEC RPS 1B cec pre certification application form files. Merely consider these particular steps.
Step 1: Select the "Get Form Now" button to begin the process.
Step 2: As soon as you've entered the editing page Form Cec Rps 1B, you should be able to find every one of the actions readily available for the document inside the upper menu.
Provide the necessary details in each one section to fill out the PDF Form Cec Rps 1B
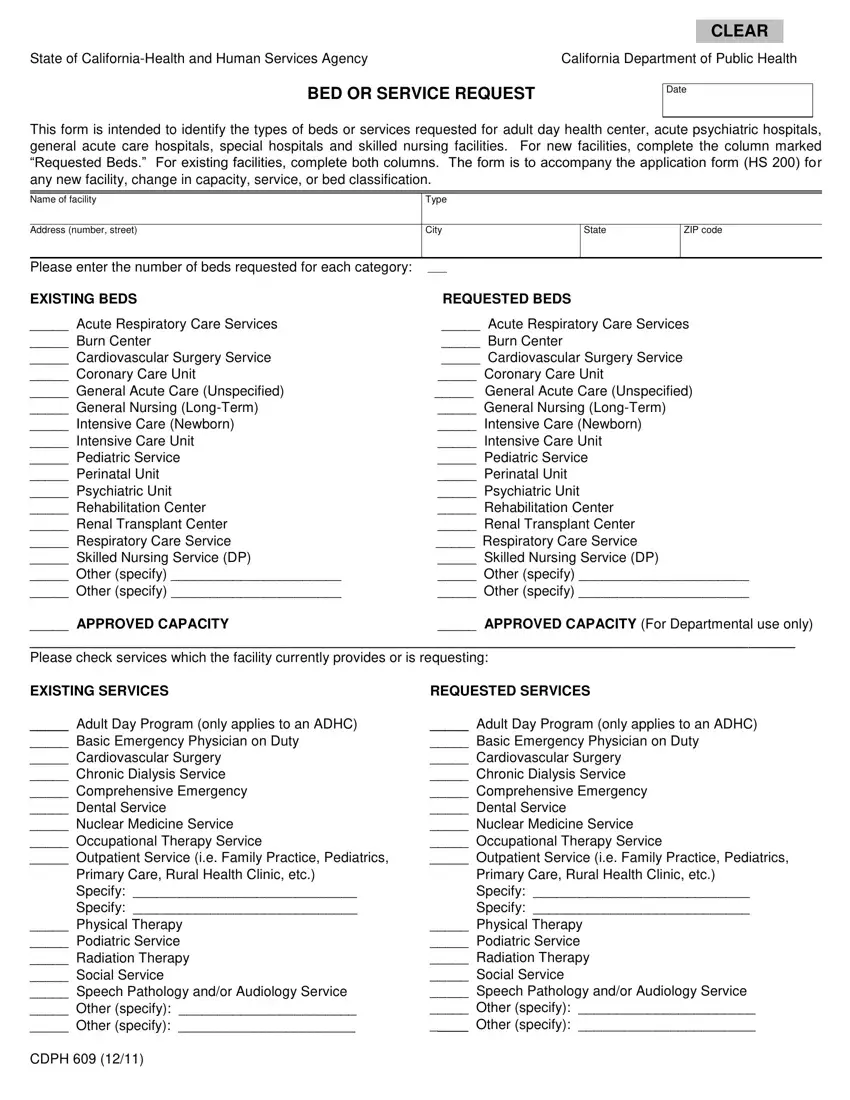
The system will expect you to prepare the Acute Respiratory Care Services, Acute Respiratory Care Services, General Acute Care Unspecified, APPROVED CAPACITY Please check, APPROVED CAPACITY For, EXISTING SERVICES, REQUESTED SERVICES, Adult Day Program only applies to, and Adult Day Program only applies to box.
It's important to put down certain data inside the field Adult Day Program only applies to, Adult Day Program only applies to, Primary Care Rural Health Clinic, Physical Therapy Podiatric, CDPH, Primary Care Rural Health Clinic, and Physical Therapy Podiatric.
Step 3: Select the Done button to make sure that your finalized document could be transferred to every gadget you use or sent to an email you indicate.
Step 4: You will need to generate as many copies of your form as you can to stay away from possible worries.
