This PDF editor allows you to complete forms. There's no need to do much to update florida medicaid documents. Only consider the next actions.
Step 1: Click the button "Get Form Here".
Step 2: So, you're on the file editing page. You can add content, edit current details, highlight particular words or phrases, place crosses or checks, insert images, sign the template, erase unwanted fields, etc.
These particular sections will help make up the PDF document:
Write down the necessary details in Living Address, Number, Street, Apt, City, Zip Code, Mailing Address, Number, Street, Apt, City, Zip Code, Telephone Number, Telephone, and Contact Person Last Other than section.
You'll be required to write down the information to let the platform fill out the section Are you a US Citizen You, Spouse, Yes, Yes, If not a citizen provide alien, You, Spouse if applying, Do you intend to remain in the, You, Spouse, Yes, Do you andor spouse have any other, You, Yes, and Yes.
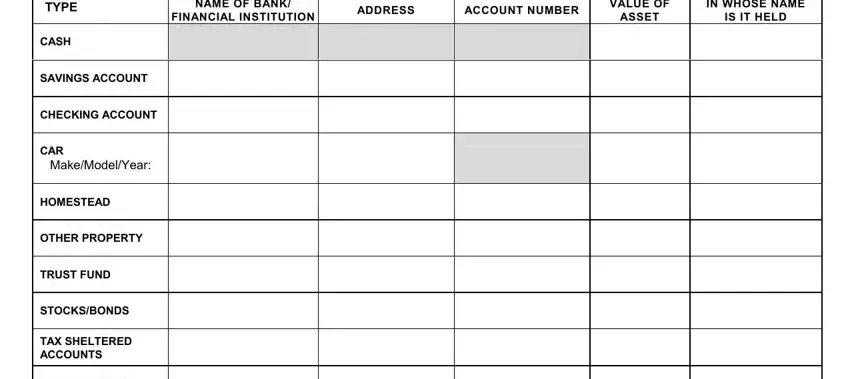
The space NAME OF BANK FINANCIAL INSTITUTION, ADDRESS, ACCOUNT NUMBER, VALUE OF ASSET, IN WHOSE NAME IS IT HELD, TYPE, CASH, SAVINGS ACCOUNT, CHECKING ACCOUNT, CAR, MakeModelYear, HOMESTEAD, OTHER PROPERTY, TRUST FUND, and STOCKSBONDS is going to be where to include each side's rights and responsibilities.
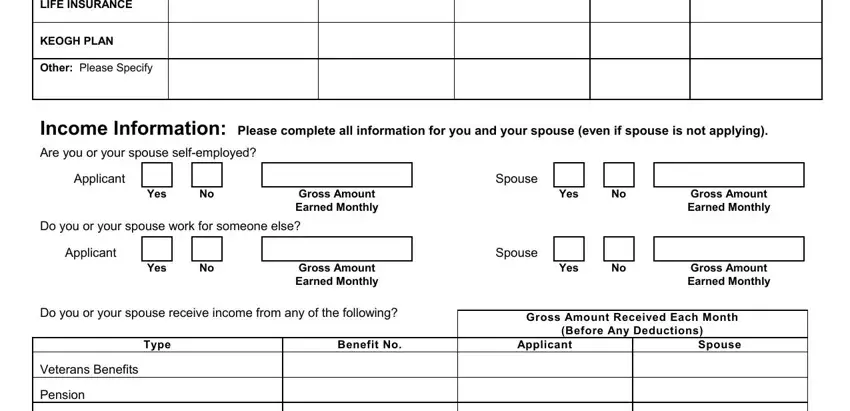
Prepare the form by checking the next areas: LIFE INSURANCE, KEOGH PLAN, Other Please Specify, Income Information Please complete, Applicant, Yes, Gross Amount Earned Monthly, Yes, Gross Amount Earned Monthly, Spouse, Do you or your spouse work for, Applicant, Yes, Gross Amount Earned Monthly, and Yes.
Step 3: Click the button "Done". Your PDF document can be transferred. You can download it to your laptop or email it.
Step 4: Create a duplicate of each file. It can save you time and help you avoid complications later on. Also, your data isn't used or viewed by us.
