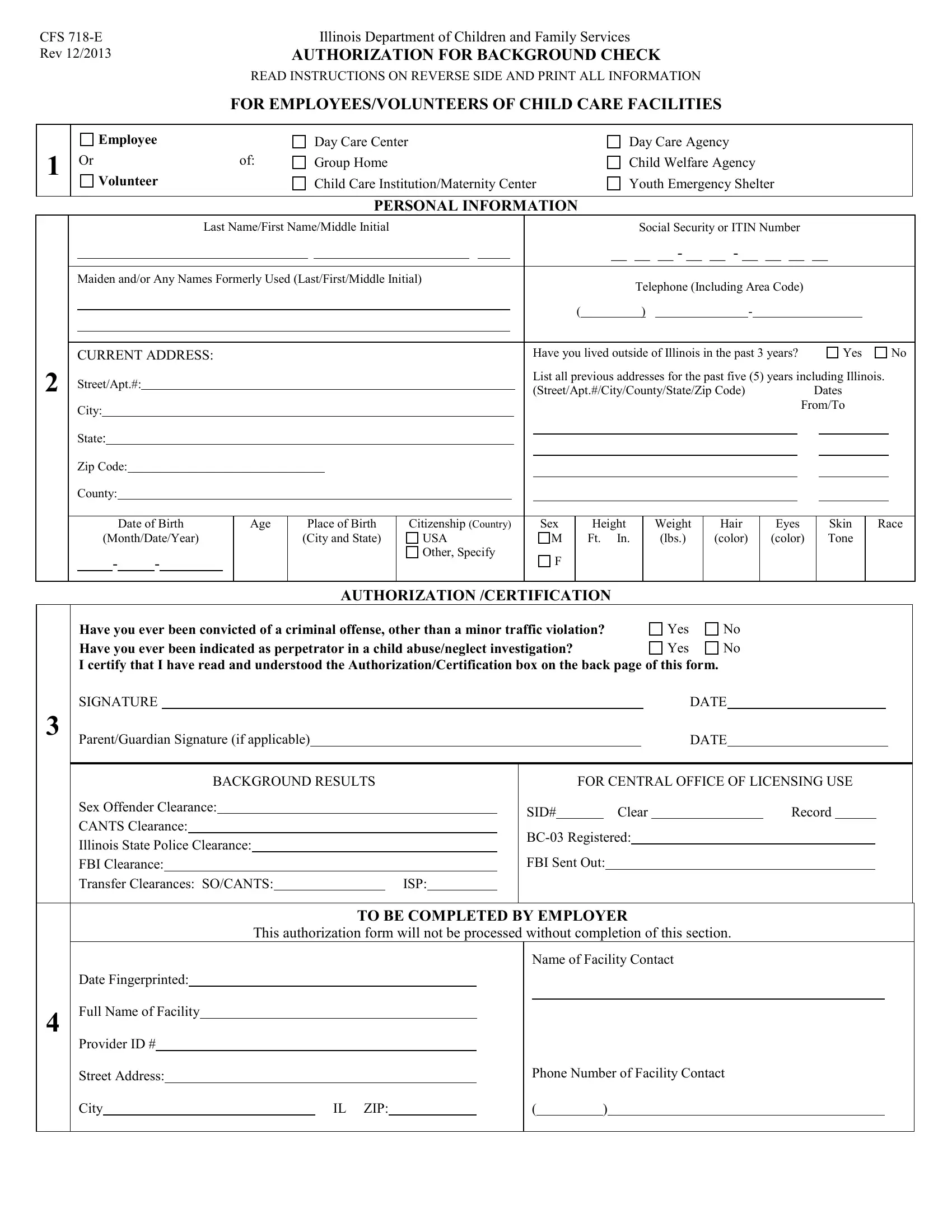
Ensuring the safety and well-being of children in care facilities is of paramount importance, making thorough background checks an essential component of the hiring process. The CFS 718-E form, developed by the Illinois Department of Children and Family Services and revised in December 2013, serves this critical function. Required for employees and volunteers, aged 13 or older, working in a variety of child care settings, this form facilitates a comprehensive evaluation of an individual's eligibility through a meticulous review of their criminal history, involvement in child abuse/neglect investigations, and other pertinent personal information. The process involves the collection of detailed personal data, including past residences and any aliases, alongside explicit consent for the Illinois Department of Children and Family Services to conduct criminal and child abuse checks. Moreover, the form mandates the disclosure of any past criminal offenses and instances of being indicated as a perpetrator in child abuse or neglect cases, ensuring a thorough assessment of potential risks. Employers play a crucial role in this process, required to verify the completeness and accuracy of the information provided before proceeding with fingerprinting. This form not only ensures the safety of children but also aids in the maintenance of a secure environment within Illinois child care facilities. Importantly, individuals have the right to contest any discrepancies found in their records, as indicated by the form's instructions, underscoring the process's fairness and transparency. The CFS 718-E form, therefore, stands as a vital tool in safeguarding vulnerable populations and upholding the standards of care expected by the community.
| Question | Answer |
|---|---|
| Form Name | Form Cfs 718E |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | CANTS, CFS, printable exemption page for chapter 7 champaign il, ISP |
