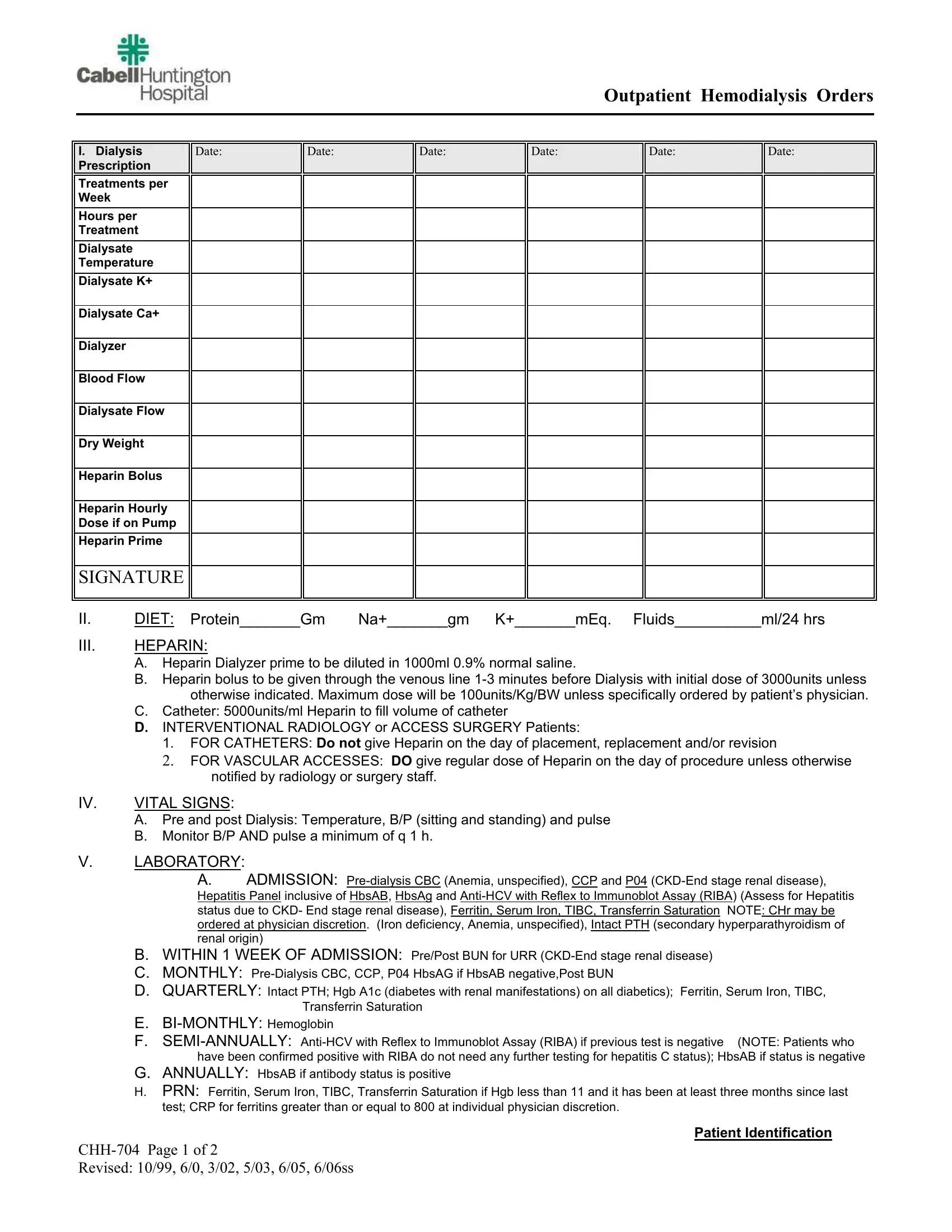
The Chh 704 form stands as a critical document in the management and treatment of patients undergoing outpatient hemodialysis, a life-sustaining procedure for individuals with severe kidney failure. This detailed form encapsulates a comprehensive dialysis prescription, including treatments per week, hours per treatment, and specifics regarding the dialysis solution used—dialysate temperature, potassium (K+), and calcium (Ca+) levels, alongside parameters for the dialyzer blood and dialysate flow. Moreover, it addresses the patient's dry weight, a vital metric for assessing fluid balance, and dosing for heparin, a medication essential for preventing blood clots during dialysis. Beyond dialysis specifics, the form encompasses diet recommendations, specifying protein, sodium, potassium, and fluid intakes, reflecting the tightly controlled dietary requirements for dialysis patients. It outlines the administration of heparin, including dosages and exceptions, vital sign monitoring protocols, and a comprehensive lab testing schedule to monitor the patient’s condition and treatment efficacy over time. Additionally, the form includes instructions for managing common complications associated with dialysis, such as hypotension and muscle cramps, and preventive measures like vaccinations. The remaining sections cover miscellaneous medical orders, from oxygen therapy to evaluations for kidney transplant eligibility, illustrating the form’s role in providing a holistic approach to patient care. By meticulously combining these elements, the Chh 704 form guides healthcare professionals in delivering standardized yet personalized dialysis treatment in an outpatient setting.
| Question | Answer |
|---|---|
| Form Name | Form Chh 704 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | CHH 0704 Outpatient Hemodialysis Orders prime date dialysis form |
