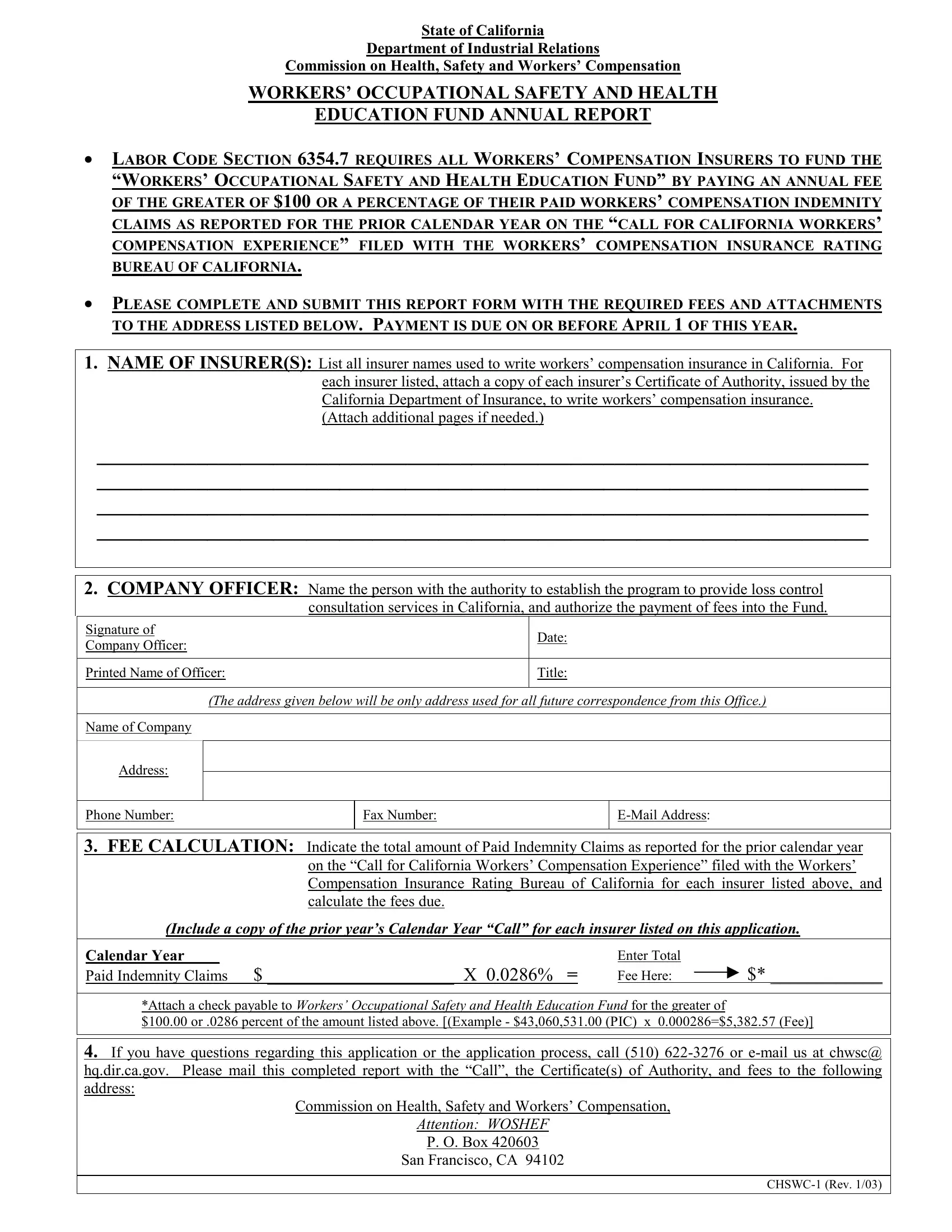
In the State of California, the Department of Industrial Relations plays a critical role in ensuring the well-being of workers through various facets, one of which includes the financial support of programs aimed at enhancing workers' knowledge on occupational safety and health. This commitment is encapsulated in the CHSWC-1 form, a mandatory document for all workers’ compensation insurers. The form is integral to the funding mechanism for the "Workers’ Occupational Safety and Health Education Fund," as mandated by Labor Code Section 6354.7. This code requires insurers to contribute an annual fee that is either a minimum of $100 or a calculated percentage based on their paid workers’ compensation indemnity claims from the previous year. This contribution is essential for nurturing a safer and more informed workforce in California. The CHSWC-1 form includes vital sections such as the insurer's identification, contact details of the company officer with authority over the program, meticulous fee calculation based on prior claims, and the process for submitting this information along with the necessary fees and attachments to the designated address. Additionally, it outlines the support available for insurers during the submission process, emphasizing the commitment of the Commission on Health, Safety and Workers' Compensation to engage and facilitate insurers in complying with this important requirement. Thus, the CHSWC-1 form serves not only as a mechanism for fund collection but also embodies a larger effort towards fostering a culture of safety and health within the occupational environment of California.
| Question | Answer |
|---|---|
| Form Name | Form Chswc 1 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | CHSWCFundFeeFor m1 form chswc 1 |
State of California
Department of Industrial Relations
Commission on Health, Safety and Workers’ Compensation
WORKERS’ OCCUPATIONAL SAFETY AND HEALTH
EDUCATION FUND ANNUAL REPORT
LABOR CODE SECTION 6354.7 REQUIRES ALL WORKERS’ COMPENSATION INSURERS TO FUND THE “WORKERS’ OCCUPATIONAL SAFETY AND HEALTH EDUCATION FUND” BY PAYING AN ANNUAL FEE OF THE GREATER OF $100 OR A PERCENTAGE OF THEIR PAID WORKERS’ COMPENSATION INDEMNITY CLAIMS AS REPORTED FOR THE PRIOR CALENDAR YEAR ON THE “CALL FOR CALIFORNIA WORKERS’ COMPENSATION EXPERIENCE” FILED WITH THE WORKERS’ COMPENSATION INSURANCE RATING BUREAU OF CALIFORNIA.
PLEASE COMPLETE AND SUBMIT THIS REPORT FORM WITH THE REQUIRED FEES AND ATTACHMENTS TO THE ADDRESS LISTED BELOW. PAYMENT IS DUE ON OR BEFORE APRIL 1 OF THIS YEAR.
1.NAME OF INSURER(S): List all insurer names used to write workers’ compensation insurance in California. For each insurer listed, attach a copy of each insurer’s Certificate of Authority, issued by the California Department of Insurance, to write workers’ compensation insurance.
(Attach additional pages if needed.)
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
______________________________________________________________________
2.COMPANY OFFICER: Name the person with the authority to establish the program to provide loss control consultation services in California, and authorize the payment of fees into the Fund.
Signature of |
|
Date: |
||
Company Officer: |
|
|||
|
|
|
||
|
|
|
|
|
Printed Name of Officer: |
|
Title: |
||
|
|
|
|
|
|
(The address given below will be only address used for all future correspondence from this Office.) |
|||
|
|
|
|
|
Name of Company |
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone Number: |
Fax Number: |
|
||
|
|
|
|
|
3.FEE CALCULATION: Indicate the total amount of Paid Indemnity Claims as reported for the prior calendar year on the “Call for California Workers’ Compensation Experience” filed with the Workers’ Compensation Insurance Rating Bureau of California for each insurer listed above, and calculate the fees due.
(Include a copy of the prior year’s Calendar Year “Call” for each insurer listed on this application.
Calendar Year ____
Paid Indemnity Claims $ ____________________ X 0.0286% =
Enter Total
Fee Here: $* ____________
*Attach a check payable to Workers’ Occupational Safety and Health Education Fund for the greater of
$100.00 or .0286 percent of the amount listed above. [(Example - $43,060,531.00 (PIC) x 0.000286=$5,382.57 (Fee)]
4.If you have questions regarding this application or the application process, call (510)
Commission on Health, Safety and Workers’ Compensation,
Attention: WOSHEF
P. O. Box 420603
San Francisco, CA 94102