

aflac dental forms can be filled in online with ease. Simply use FormsPal PDF editing tool to get it done promptly. The tool is constantly upgraded by us, acquiring useful functions and turning out to be much more versatile. Getting underway is effortless! All you need to do is take these easy steps down below:
Step 1: First of all, open the tool by pressing the "Get Form Button" at the top of this webpage.
Step 2: After you launch the PDF editor, you'll notice the document prepared to be completed. Other than filling out different blank fields, you could also perform several other things with the form, such as writing custom text, modifying the original textual content, inserting illustrations or photos, putting your signature on the form, and more.
This PDF will require specific data to be typed in, hence you should take your time to enter exactly what is asked:
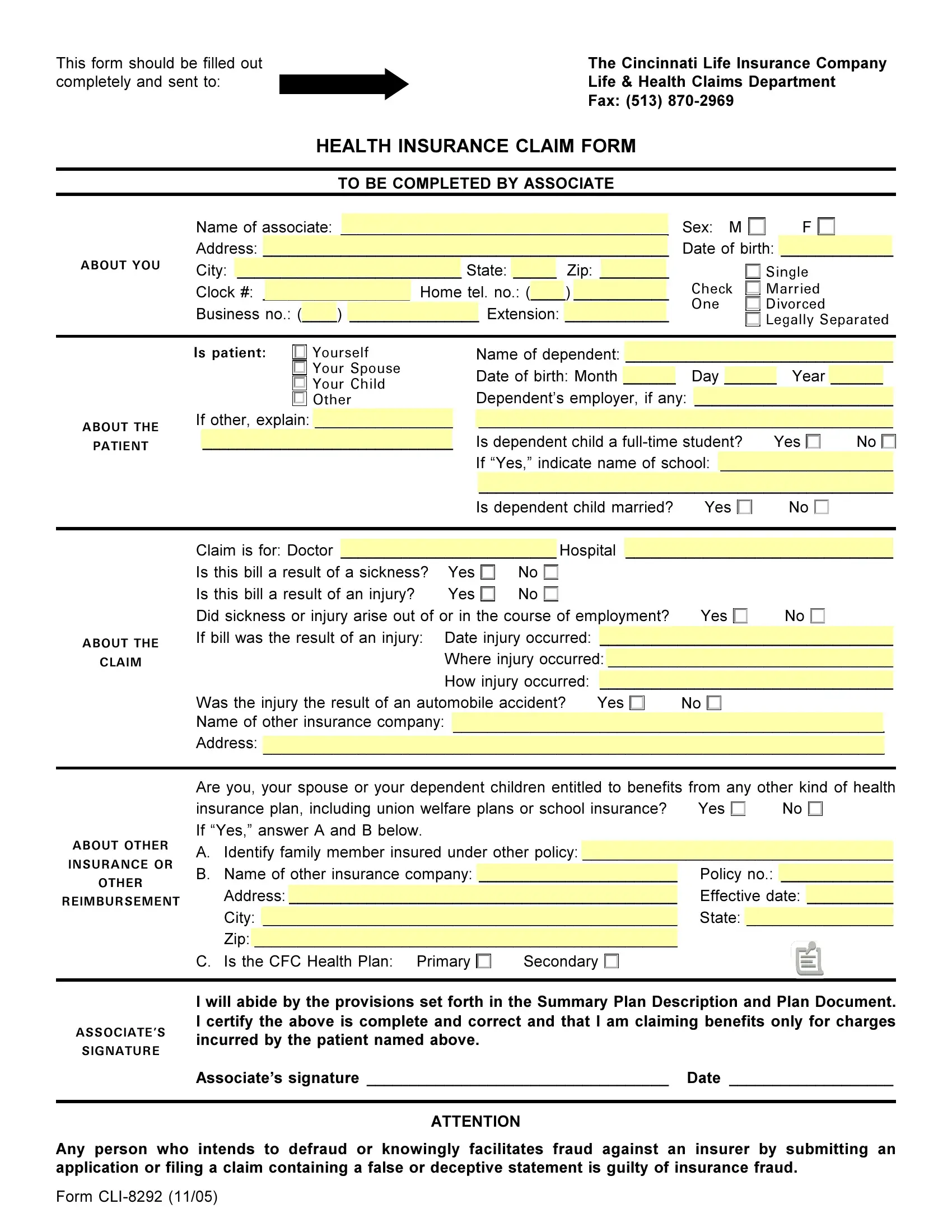
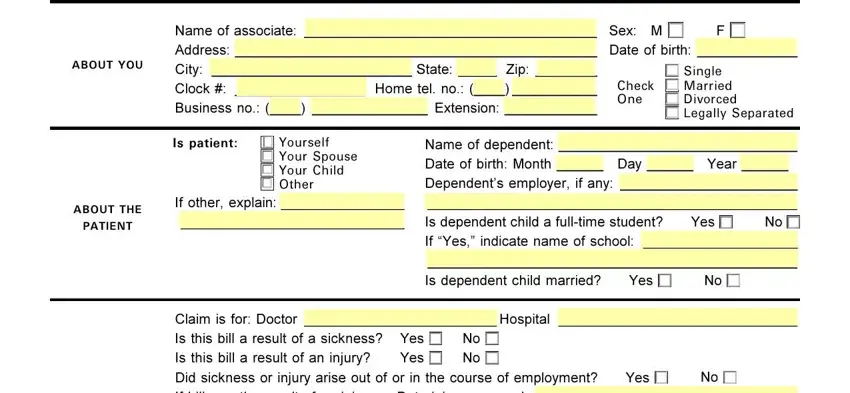
1. Start completing your aflac dental forms with a selection of essential blanks. Gather all the information you need and make certain absolutely nothing is omitted!
2. The third step is usually to submit these blanks: Claim is for Doctor Hospital Is, Was the injury the result of an, Yes, Are you your spouse or your, Yes, ABOUT THE, CLAIM, ABOUT OTHER, INSURANCE OR, OTHER, REIMBURSEMENT, C Is the CFC Health Plan Primary, Secondary, and I will abide by the provisions set.
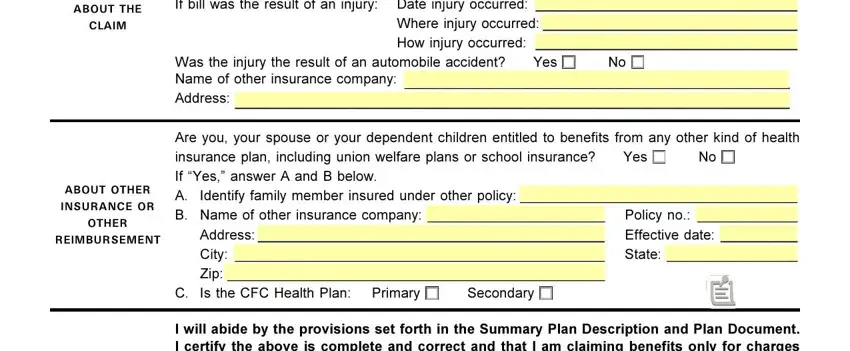
Always be extremely careful while filling out Yes and Claim is for Doctor Hospital Is, since this is the section where most users make errors.
Step 3: Right after looking through the form fields, click "Done" and you're good to go! Grab your aflac dental forms as soon as you subscribe to a free trial. Quickly view the pdf file inside your FormsPal account page, together with any modifications and adjustments being conveniently saved! We don't share or sell the information you enter when completing forms at our website.