
You'll be able to prepare Form CMS 10123-NOMNC pdf easily in our PDFinity® online PDF tool. Our expert team is relentlessly working to expand the editor and make it even better for people with its cutting-edge features. Take full advantage of the current progressive opportunities, and find a myriad of unique experiences! To get the process started, go through these simple steps:
Step 1: Firstly, access the pdf editor by clicking the "Get Form Button" above on this page.
Step 2: After you launch the tool, you will get the document all set to be filled out. Apart from filling in different blanks, you may also perform some other actions with the PDF, namely writing custom words, changing the initial textual content, inserting images, placing your signature to the form, and much more.
Completing this document needs attentiveness. Make sure that each and every blank field is done accurately.
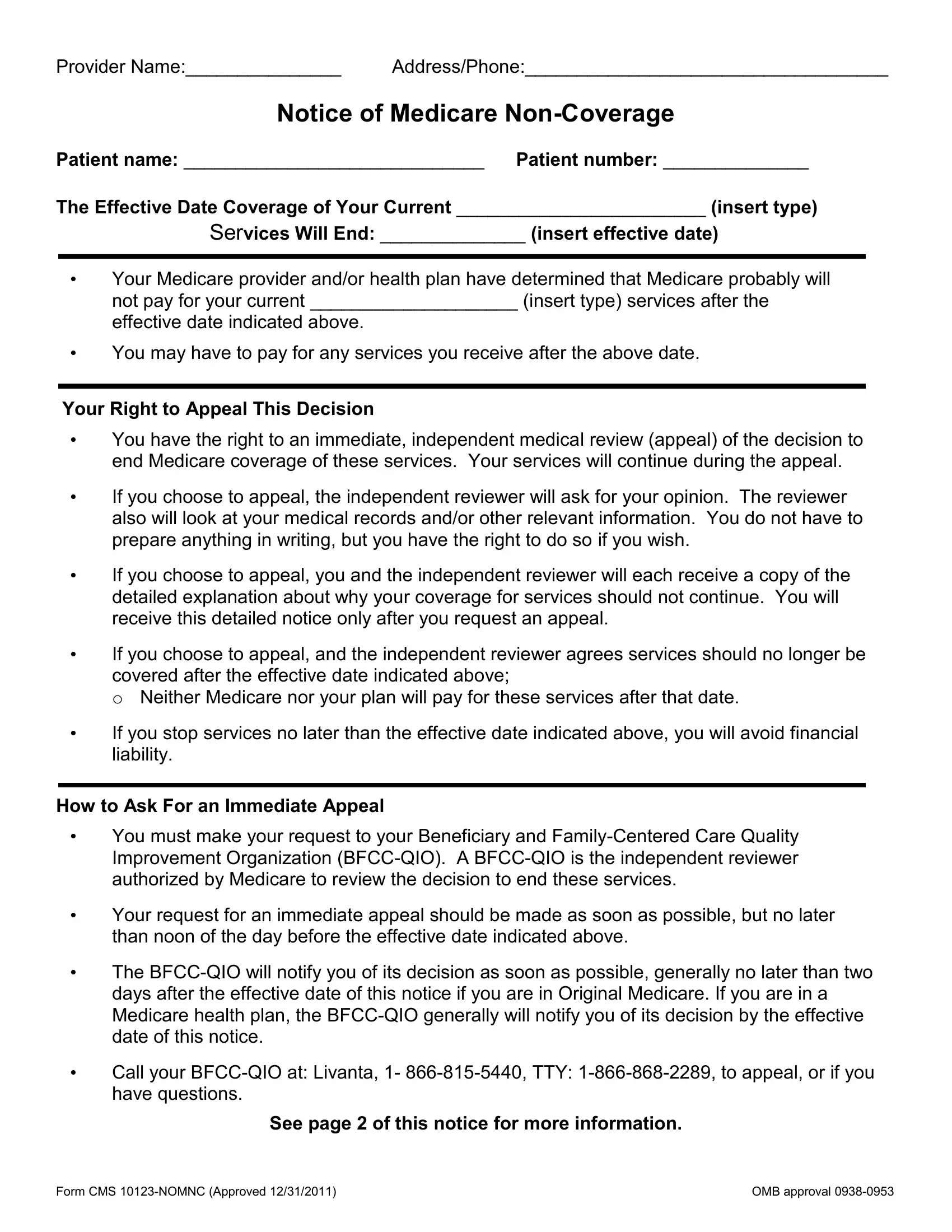
1. It's important to complete the Form CMS 10123-NOMNC pdf accurately, thus be mindful while filling out the segments including these blanks:
2. Once your current task is complete, take the next step – fill out all of these fields - Additional Information Optional, Please sign below to indicate you, Signature of Patient or, and Date with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
It's easy to get it wrong when completing your Please sign below to indicate you, so make sure you look again before you'll finalize the form.
Step 3: Make sure that your details are correct and then click "Done" to conclude the process. Acquire your Form CMS 10123-NOMNC pdf as soon as you join for a free trial. Instantly use the pdf file in your personal cabinet, with any edits and changes all kept! FormsPal guarantees protected document editing with no data recording or any type of sharing. Be assured that your information is in good hands here!