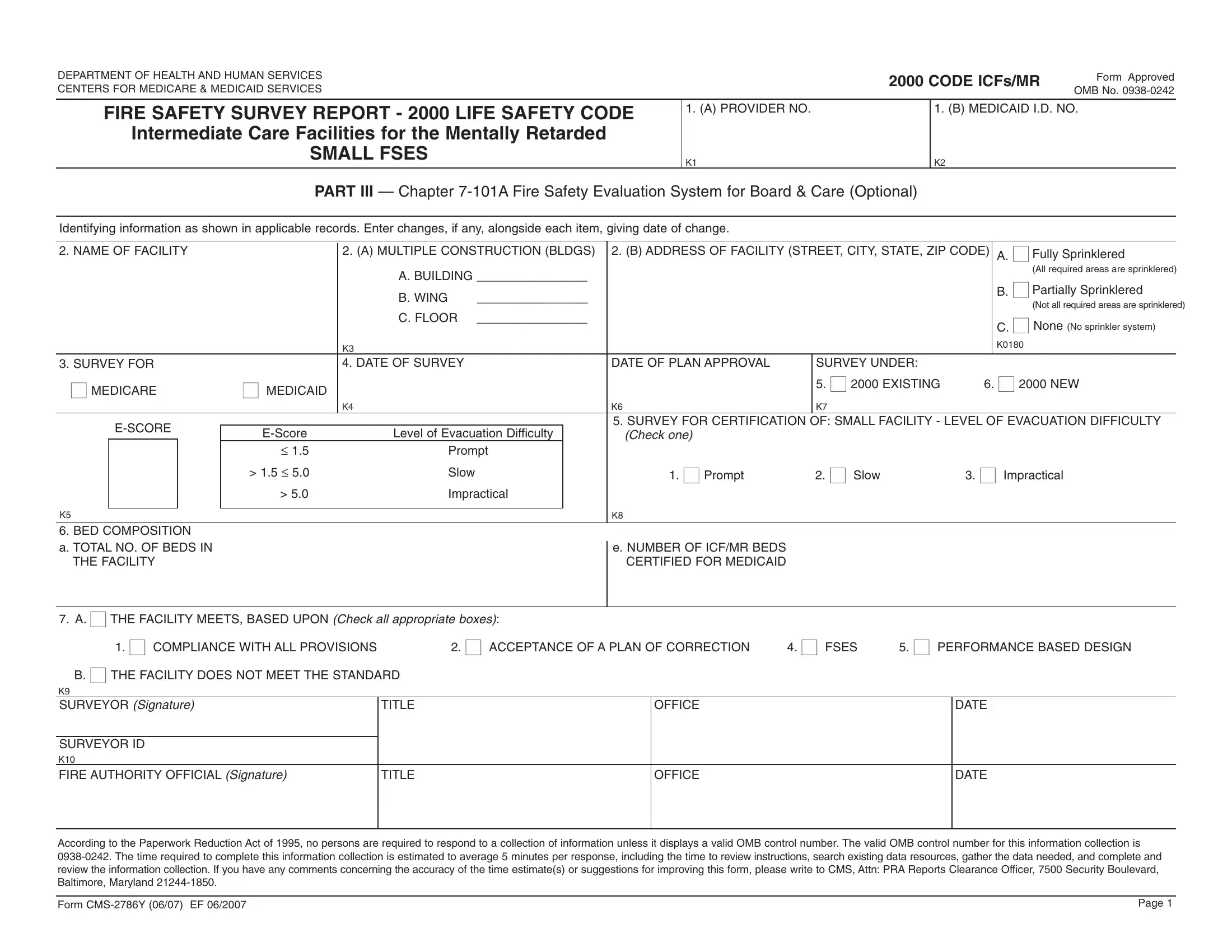
Ensuring the safety and welfare of residents in intermediate care facilities for the mentally retarded (ICFs/MR) is a paramount concern that is addressed through meticulous regulatory requirements and oversight. One critical aspect of this oversight involves the CMS 2786Y form, an instrument developed by the Department of Health and Human Services and the Centers for Medicare & Medicaid Services. This form plays a pivotal role in conducting fire safety surveys, thereby aligning facilities with the stringent standards set by the 2000 Life Safety Code. It encompasses a comprehensive assessment spanning several key areas: the verification of functional sprinkler systems, whether fully or partially installed, or the absence thereof; the rigorous evaluation of facilities through dates of surveys, plans approval, and certification types for both old and new constructs; the assessment of evacuation difficulty levels; and, fundamentally, determining a facility's compliance or non-compliance with the Life Safety Code. The form also facilitates a methodical fire safety evaluation system for small facilities, potentially accommodating 16 or fewer residents, thus presenting a structured approach to achieving or maintaining fire safety standards. Evaluated parameters include construction features, hazard zones, fire alarm effectiveness, smoke detection, automatic sprinklers, and interior finish, among others, pinpointing areas necessitating improvement or signifying compliance and safety. This detailed evaluation concludes with equivalent safety measures and mandatory safety requirements, effectively guiding facilities toward the required levels of fire protection and preparedness.
| Question | Answer |
|---|---|
| Form Name | Form Cms 2786Y |
| Form Length | 6 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 30 sec |
| Other names | CMS2786Y fses fillable form |
DEPARTMENT OF HEALTH AND HUMAN SERVICES CENTERS FOR MEDICARE & MEDICAID SERVICES
2000 CODE ICFs/MR
Form Approved OMB No.
FIRE SAFETY SURVEY REPORT - 2000 LIFE SAFETY CODE |
1. (A) PROVIDER NO. |
1. (B) MEDICAID I.D. NO. |
|
|
|
Intermediate Care Facilities for the Mentally Retarded |
|
|
SMALL FSES |
K1 |
K2 |
|
PART III — Chapter
Identifying information as shown in applicable records. Enter changes, if any, alongside each item, giving date of change.
2. NAME OF FACILITY |
|
2. (A) MULTIPLE CONSTRUCTION (BLDGS) |
2. (B) ADDRESS OF FACILITY (STREET, CITY, STATE, ZIP CODE) |
A. ■ Fully Sprinklered |
|
||||||
|
|
|
|
A. BUILDING ________________ |
|
|
|
(All required areas are sprinklered) |
|||
|
|
|
|
|
|
|
B. ■ Partially Sprinklered |
||||
|
|
|
|
B. WING |
________________ |
|
|
|
|||
|
|
|
|
|
|
|
(Not all required areas are sprinklered) |
||||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
C. FLOOR |
________________ |
|
|
|
C. ■ None (No sprinkler system) |
||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
K3 |
|
|
|
|
|
K0180 |
|
|
|
|
|
|
|
|
|
|
|
|
|
3. SURVEY FOR |
|
4. DATE OF SURVEY |
|
|
DATE OF PLAN APPROVAL |
SURVEY UNDER: |
|
|
|
||
■ MEDICARE |
■ MEDICAID |
|
|
|
|
5. ■ 2000 EXISTING |
6. ■ 2000 NEW |
||||
|
|
|
|
|
|
|
|
||||
|
|
|
|
K4 |
|
|
K6 |
K7 |
|
|
|
|
|
|
|
|
5. SURVEY FOR CERTIFICATION OF: SMALL FACILITY - LEVEL OF EVACUATION DIFFICULTY |
||||||
|
Level of Evacuation Difficulty |
|
(Check one) |
|
|
|
|
||||
|
|
|
|
|
|
|
|
||||
|
|
|
≤ 1.5 |
Prompt |
|
|
|
|
|
|
|
|
|
|
> 1.5 ≤ 5.0 |
Slow |
|
|
1. ■ Prompt |
2. ■ Slow |
3. ■ Impractical |
||
|
|
|
> 5.0 |
Impractical |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
K5 |
|
|
|
|
K8 |
|
|
|
|
||
6. BED COMPOSITION
a. TOTAL NO. OF BEDS IN THE FACILITY
e. NUMBER OF ICF/MR BEDS CERTIFIED FOR MEDICAID
7. A. ■ THE FACILITY MEETS, BASED UPON (Check all appropriate boxes):
1. ■ COMPLIANCE WITH ALL PROVISIONS |
|
2. ■ ACCEPTANCE OF A PLAN OF CORRECTION |
4. ■ FSES |
5. ■ PERFORMANCE BASED DESIGN |
||
B. ■ THE FACILITY DOES NOT MEET THE STANDARD |
|
|
|
|
|
|
K9 |
|
|
|
|
|
|
SURVEYOR (Signature) |
TITLE |
|
OFFICE |
|
|
DATE |
|
|
|
|
|
|
|
SURVEYOR ID |
|
|
|
|
|
|
K10 |
|
|
|
|
|
|
FIRE AUTHORITY OFFICIAL (Signature) |
TITLE |
|
OFFICE |
|
|
DATE |
|
|
|
|
|
|
|
According to the Paperwork Reduction Act of 1995, no persons are required to respond to a collection of information unless it displays a valid OMB control number. The valid OMB control number for this information collection is
Form |
Page 1 |
Fire Safety Evaluation Worksheet for a
Small Facility
Facility Identification ___________________________________________________________________________________
Evaluator _________________________________________ |
Date __________________________________________ |
(Complete one worksheet for each individual residence or apartment used as a board and care home. A small facility normally means a capacity for 16 or fewer residents.)
First complete Worksheet 7.3.1. Continue with Worksheets 7.3.3, 7.3.4, 7.3.5 and 7.3.6. Then return to this page to obtain the Equivalency Conclusions.
TURN TO NEXT PAGE
Part 1E. Equivalency Conclusions.
Complete Worksheets 7.3.1 through 7.3.6 before doing this part.
1.■ All of the checks in Worksheet 7.3.7 are in the “YES” column. The level of fire safety is at least equivalent to that prescribed by the Life Safety Code.*
2.■ One or more of the checks in Worksheet 7.3.7 is in the “NO” column. The level of fire safety is not shown by this system to be equivalent to that prescribed for small dwelling units.
*The equivalency covered by this worksheet includes the majority of considerations covered by the Life Safety Code. There are a few considerations that are not evaluated by this method. These must be considered separately. These additional considerations are covered in the “Facility Fire Safety Requirements Worksheet.” One copy of this separate worksheet is to be completed for each facility.
Form |
Page 2 |

Figure 7.3 Worksheets for evaluating fire safety in a small facility.
WORKSHEET 7.3.1 COVER SHEET
Fire Safety Evaluation Worksheet for Small Facility
____________________________________________________________________
WORKSHEET 7.3.2 SAFETY PARAMETER VALUES — SMALL FACILITY
Safety Parameters |
|
|
|
|
|
|
|
|
|
|
Parameter Values |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
1. Construction/ |
|
Exposed Structural |
|
|
|
|
Protected |
|
|
|
|
|
|
|
Protected |
|||||||||||||||||
Fire Resistance |
|
|
Members |
|
|
|
|
15 min |
|
|
|
|
|
|
|
|
1 hr |
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
0 |
|
|
|
|
|
|
|
|
|
1 |
|
|
|
|
|
|
|
|
|
|
3 |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
2. Hazardous Areas |
|
Double Deficiency |
|
|
Single Deficiency |
|
|
|
|
None or No Deficiency |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
3. Manual Fire Alarm |
None or Incomplete |
|
w/o F.D. Notification |
|
|
|
w/ F.D. Notification |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
0 |
|
|
|
|
|
|
|
|
|
1 |
|
|
|
|
|
|
|
|
|
|
2 |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
4. Smoke Detection |
|
|
|
|
|
|
|
|
|
|
|
|
|
Warning to All Bedrooms |
|
|
|
|
|
|
|
|
||||||||||
and Alarm |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
None or |
|
|
|
Single Lev. Det./ |
|
|
|
|
|
|
|
|
|
Every Lev. Plus |
|
|
Total Coverage |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
Incomplete |
|
|
Limited Warning |
Every Lev. Det.e |
|
Det. in Each Bdrm. |
|
|
|
|
System |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
|
|
|
|
2 |
|
|
|
|
|
|
|
3(4)f |
|
|
|
|
|
|
4 |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
5. Automatic Sprinklers |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
Nonsprinklered |
|
|
Standard Sprinklers |
|
|
|
|
Residential Sprinklers |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
0 |
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
|
|
|
10 |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
6. Interior Finish |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
>75 to <200 |
|
|
|
>25 to <75 |
|
|
|
|
|
|
|
<25 |
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
7. Separation of |
|
Unprotected |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Sleeping Rooms |
Vertical Openings |
|
|
|
|
|
|
|
Protected Vertical Openings |
d |
|
|
||||||||||||||||||||
(from other levels |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
and from corridors) |
None or |
|
Smoke |
|
Smoke |
|
None or |
|
Smoke |
|
|
|
|
|
1/2 hr |
|
Smoke Res. |
|
1/2 hr |
|||||||||||||
|
|
|
Resisting |
|
Resisting |
|
|
|
|
|
|
|
Auto |
|
|
w/ Door |
|
w/ Door |
||||||||||||||
|
|
Incomp. |
|
w/o Closers |
|
w/ Closers |
|
Incomp. |
|
Resisting |
|
1/2 hr. |
|
Closing |
|
|
Closer |
|
Closer |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
0(0)c |
|
|
|
0 |
|
|
|
1(0)a |
|
2(0)a |
|
|
1 |
|
|
2(1)a |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
8. Means |
Means of |
|
<2 Remote Routes |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
of Escape |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Escape on |
w/o Alt. |
|
|
w/ Alt. |
|
2 Remote Routes |
|
|
2 Remote Routes |
Direct Exit from |
||||||||||||||||||||||
|
All Sleeping |
Means |
|
|
Means |
|
Unseparated |
|
|
|
Separated |
|
|
|
|
Each Bdrm. |
||||||||||||||||
|
Levels |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
0 |
|
|
|
|
1(0)b |
|
|
|
|
2(0)b |
|
|
|
|
|
|
3(0)b |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
Means of |
|
Primary Route Not Protected |
|
|
|
|
|
|
|
Primary Route Protected |
|
|
|||||||||||||||||||
|
Escape Not |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
<2 Remote Routes |
|
|
|
|
|
|
|
|
< 2 Remote Routes |
|
|
|
|
|
|
|
|
||||||||||||||
|
on All |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sleeping |
w/o Alt. |
|
w/ Alt. |
|
2 Remote |
|
|
|
w/o Alt |
|
|
w/ Alt. |
|
|
|
|
|
2 Remote |
|||||||||||||
|
Means |
|
Means |
|
Routes |
|
|
|
|
Means |
|
|
Means |
|
|
|
|
|
|
|
Routes |
|||||||||||
|
Levels |
|
|
|
|
|
|
|
0 |
|
|
|
|
|
|
0 |
|
|
|
|
|
|
|
2(0)b |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NOTES:
a |
Use ( ) if Parameter 1 is 0 and Parameter 5 is 0. |
|
buse (0) if Parameter 7 is based on a “none or incomplete” situation.
cUse (0) if door is 20 minute and has automatic closer.
dConsider a single level building as having protected vertical openings.
eEvery level detection is permitted to be omitted with a
fUse (4) in existing buildings if detection in each bedroom and
(For use with NFPA
Form |
Page 3 |
|
Building |
|
Identification |
_________________________________________ |
|
_________________________________ |
|
DateEvaluator
Figure 7.3 Continued
WORKSHEET 7.3.3 INDIVIDUAL SAFETY EVALUATIONS — SMALL FACILITY
|
|
|
|
|
|
General |
|
|
Fire Control |
Egress |
Refuge |
Fire Safety |
|
|
Safety Parameters |
(S1) |
(S2) |
(S3) |
(S4) |
|
|
|
|
|
|
|
|
1. |
Construction |
|
|
|
|
|
|
|
|
|
|
|
|
2. |
Hazardous Areas |
|
|
|
|
|
|
|
|
|
|
|
|
3. |
Manual Fire Alarm |
2 = |
(See note) |
|
|
|
|
|
|
|
|
|
|
4. |
Smoke Detection and Alarm |
2 = |
|
|
||
|
|
|
|
|
|
|
5. |
Automatic Sprinklers |
|
|
|
|
|
|
|
|
|
|
|
|
6. |
Interior Finish |
2 = |
|
|
|
|
|
|
|
|
|
|
|
7. |
Separation of Sleeping Rooms |
|
|
|
|
|
|
|
|
|
|
|
|
8. |
Means of Escape |
|
|
|
|
|
|
|
|
|
|
|
|
|
Total |
S1= |
S2= |
S3= |
S4= |
|
NOTE: Maximum value of manual fire alarm for means of escape is 1.
WORKSHEET 7.3.4 MANDATORY SAFETY REQUIREMENTS
|
Control |
|
|
Egress |
Refuge |
|
General Fire Safety |
||||
Level of Evacuation |
Requirements (Sa) |
Requirements (Sb) |
Requirements (Sc) |
Requirements (Sd) |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
Difficulty |
New |
|
Exist. |
New |
|
Exist. |
New |
|
Exist. |
New |
Exist. |
|
|
|
|
|
|
|
|
|
|
|
|
Prompt |
10(1/2)a |
|
0 |
5(5)a |
|
4 |
11(21/2)a |
|
2 |
7(2)a |
1 |
Slow |
10 |
|
2 |
9 |
|
7 |
11 |
|
4 |
11 |
7 |
Slowb |
|
|
1 |
|
|
6 |
|
|
2 |
|
5 |
Impractical |
10 |
|
8 |
10 |
|
9 |
11 |
|
9 |
12 |
10 |
|
|
|
|
|
|
|
|
|
|
|
|
a |
Use ( ) for small board and care facility conversion serving eight or fewer residents with an evacuation capability rating |
|
|
|
of “prompt.” |
bIn existing buildings only, use these mandatory safety requirements if evacuation time is 8 minutes or less or if the evacuation capability score is 3 or less as determined by Chapter 6.
(For use with NFPA
Form |
Page 4 |