
CONNECTICUT can be filled in online without difficulty. Simply try FormsPal PDF editor to finish the job in a timely fashion. Our tool is continually evolving to provide the best user experience attainable, and that's thanks to our commitment to constant improvement and listening closely to feedback from users. Starting is easy! All you need to do is take the next simple steps directly below:
Step 1: Access the PDF file inside our editor by clicking on the "Get Form Button" in the top part of this webpage.
Step 2: The tool will give you the capability to work with your PDF file in many different ways. Enhance it by writing customized text, adjust what is already in the document, and place in a signature - all within a few clicks!
This PDF doc will need some specific details; to guarantee correctness, be sure to take heed of the tips below:
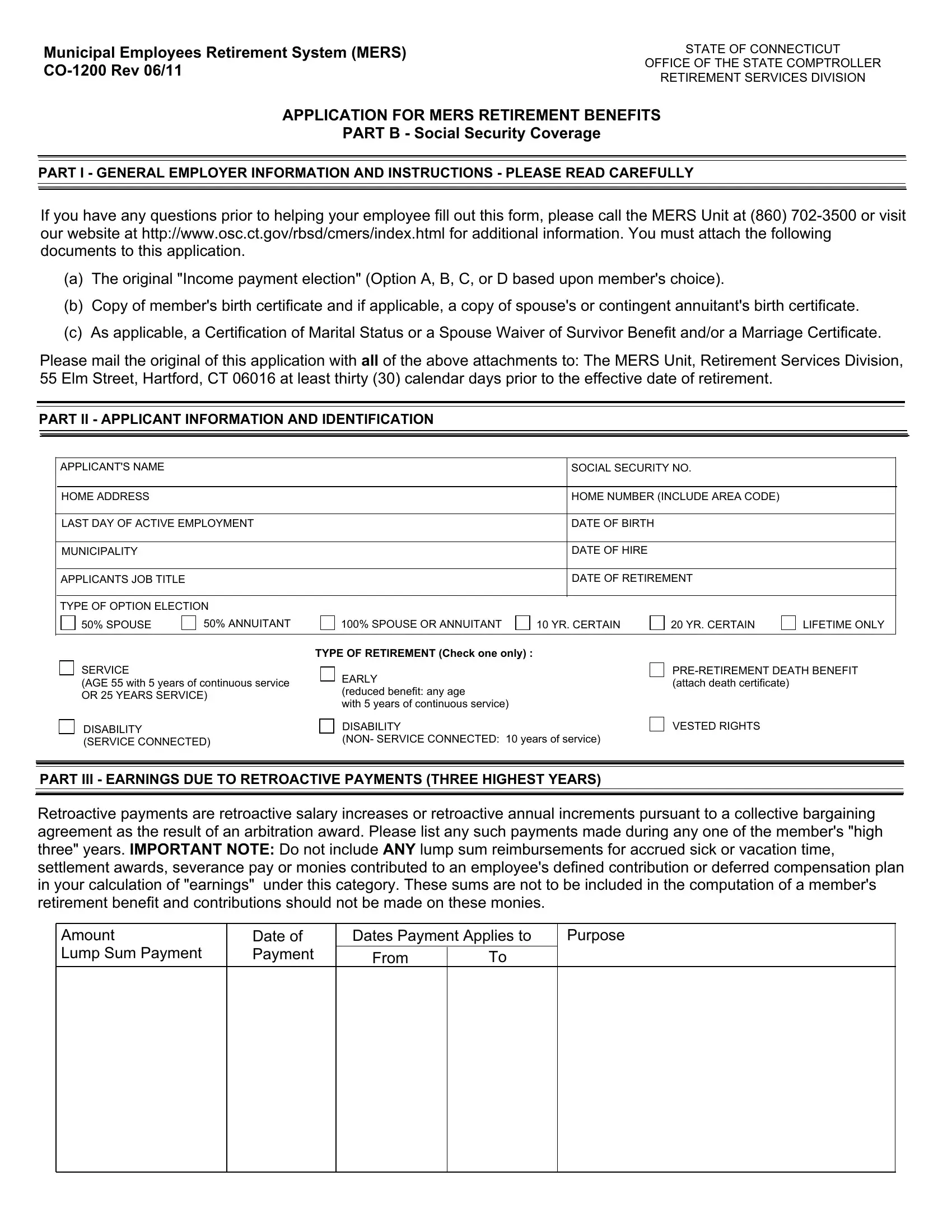
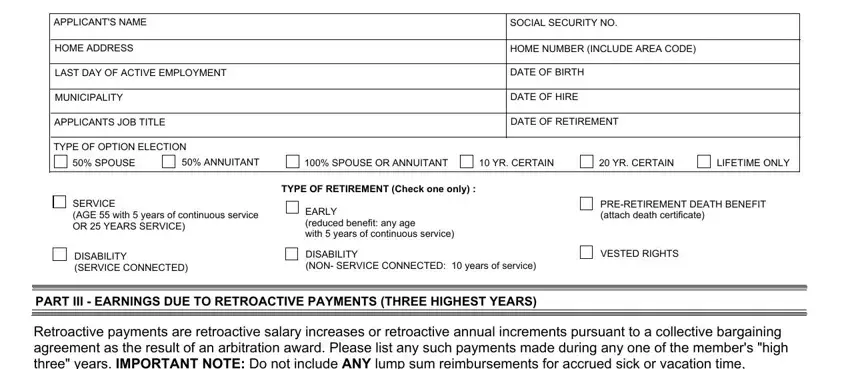
1. Fill out your CONNECTICUT with a group of necessary blanks. Consider all the necessary information and ensure nothing is neglected!
2. After the previous part is done, you're ready to insert the required details in Amount Lump Sum Payment, Date of Payment, and From in order to move forward further.
3. Completing Provide separate and chronological, From, PART V DISABILITY RETIREMENT, If you are applying for a, CO Members Statement Application, CO Physicians Statement, CO Employers Statement, and It is your responsibility to is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
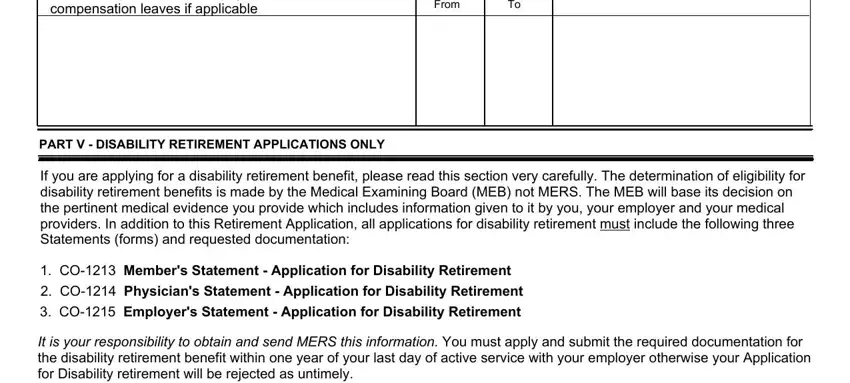
As to PART V DISABILITY RETIREMENT and CO Members Statement Application, be sure that you take a second look here. The two of these are definitely the most important fields in this page.
4. Filling in If you applied for a service, If you are eligible do you wish, Have you applied for or currently, PART VI SIGNATURES, Yes, I acknowledge that prior to, EFFECTIVE RETIREMENT DATE, APPLICANTS SIGNATURE, DATE, On behalf of the employer I hereby, AUTHORIZED EMPLOYER SIGNATURE, TITLE, DATE, EMPLOYER CONTACT PRINT NAME, and EMPLOYER CONTACT TELEPHONE NUMBER is vital in this fourth step - ensure to invest some time and fill in each and every field!
Step 3: Be certain that your details are right and then just click "Done" to continue further. Obtain your CONNECTICUT as soon as you register here for a 7-day free trial. Easily view the pdf form inside your FormsPal account, along with any modifications and adjustments automatically preserved! FormsPal provides safe document editor devoid of personal data record-keeping or sharing. Be assured that your data is in good hands with us!