Ensuring timely and appropriate healthcare for children in foster or treatment foster care is a significant responsibility that requires clear communication and consent mechanisms. The DCF F CFS0997 form, developed by the Department of Children and Families (DCF), Division of Safety and Permanence, serves as a crucial tool in facilitating this aspect of childcare. This form, which submission is voluntary, plays a vital role in aiding caregivers by providing consent for routine and emergency medical services for the child under their care. By completing the form, a parent or guardian enables the child placing agency or its designee to make informed decisions concerning the child's medical needs, including dental and nonemergency treatments, and to act swiftly in emergency situations where the guardian may not be immediately reachable. It is designed to ensure that all medical actions taken are under the supervision of duly licensed professionals. Furthermore, the form collects essential personal information, subject to privacy laws, used to identify the child and ensure their health care needs are adequately met. It also provides space for specifying exemptions and additional information, ensuring personalized care tailored to the child's unique needs. Additionally, it acknowledges the potential for the use of provided information for secondary purposes, adhering to the privacy regulations outlined in Wisconsin Statutes. The form's structure underscores the comprehensive approach taken to safeguard the health of children in foster care, focusing on preparatory consent, emergency procedures, and guardian's information, thereby embedding a systematic process for healthcare consent within the foster care system.
| Question | Answer |
|---|---|
| Form Name | Form Dcf F Cfs0997 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | yyyy, DCF-F-CFS0997, nonemergency, immunizations |
DEPARTMENT OF CHILDREN AND FAMILIES
Division of Safety and Permanence
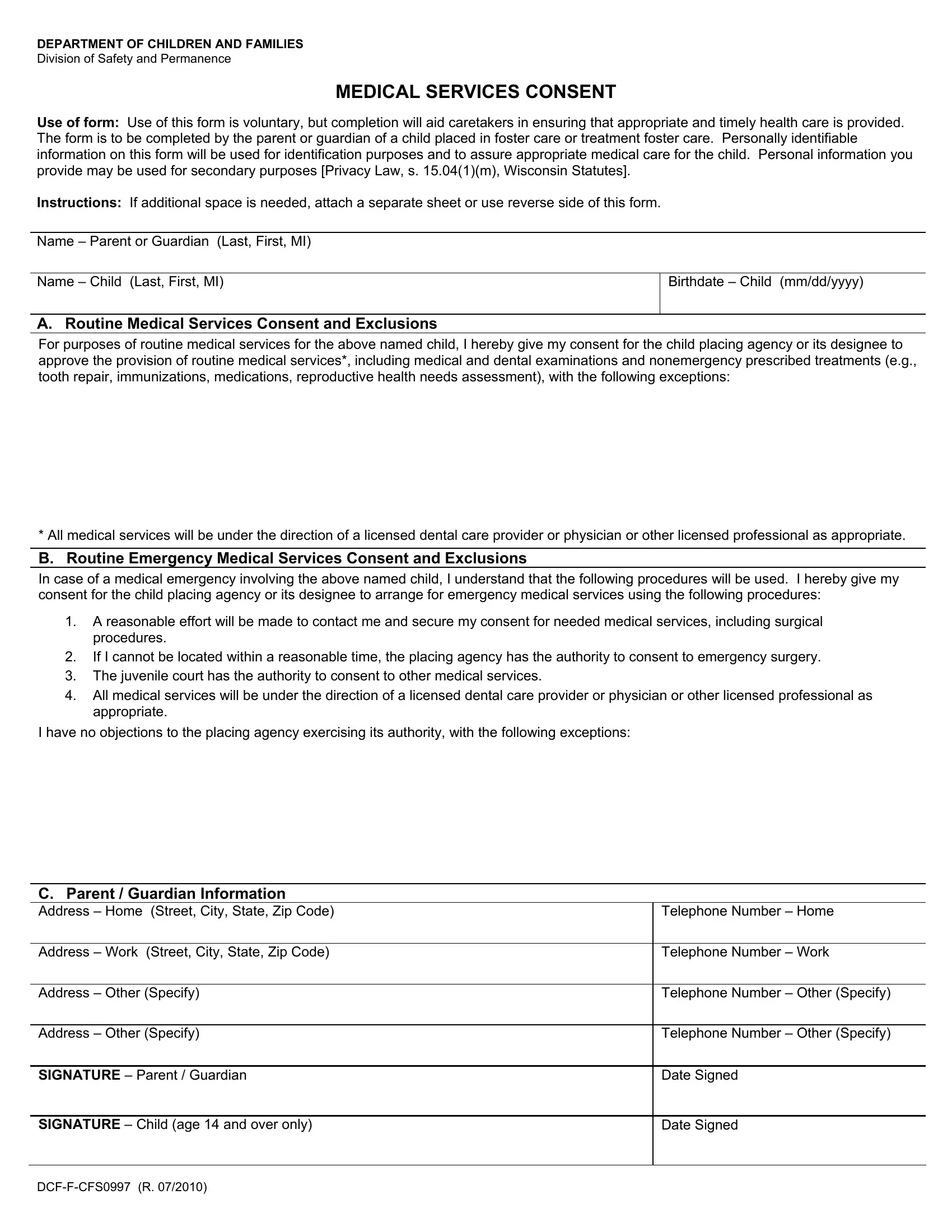
MEDICAL SERVICES CONSENT
Use of form: Use of this form is voluntary, but completion will aid caretakers in ensuring that appropriate and timely health care is provided. The form is to be completed by the parent or guardian of a child placed in foster care or treatment foster care. Personally identifiable information on this form will be used for identification purposes and to assure appropriate medical care for the child. Personal information you provide may be used for secondary purposes [Privacy Law, s. 15.04(1)(m), Wisconsin Statutes].
Instructions: If additional space is needed, attach a separate sheet or use reverse side of this form.
Name – Parent or Guardian (Last, First, MI)
Name – Child (Last, First, MI)
Birthdate – Child (mm/dd/yyyy)
A. Routine Medical Services Consent and Exclusions
For purposes of routine medical services for the above named child, I hereby give my consent for the child placing agency or its designee to approve the provision of routine medical services*, including medical and dental examinations and nonemergency prescribed treatments (e.g., tooth repair, immunizations, medications, reproductive health needs assessment), with the following exceptions:
* All medical services will be under the direction of a licensed dental care provider or physician or other licensed professional as appropriate.
B. Routine Emergency Medical Services Consent and Exclusions
In case of a medical emergency involving the above named child, I understand that the following procedures will be used. I hereby give my consent for the child placing agency or its designee to arrange for emergency medical services using the following procedures:
1.A reasonable effort will be made to contact me and secure my consent for needed medical services, including surgical procedures.
2.If I cannot be located within a reasonable time, the placing agency has the authority to consent to emergency surgery.
3.The juvenile court has the authority to consent to other medical services.
4.All medical services will be under the direction of a licensed dental care provider or physician or other licensed professional as appropriate.
I have no objections to the placing agency exercising its authority, with the following exceptions:
C. Parent / Guardian Information
Address – Home (Street, City, State, Zip Code)
Telephone Number – Home
Address – Work (Street, City, State, Zip Code)
Telephone Number – Work
Address – Other (Specify)
Telephone Number – Other (Specify)
Address – Other (Specify)
Telephone Number – Other (Specify)
SIGNATURE – Parent / Guardian
Date Signed
SIGNATURE – Child (age 14 and over only)
Date Signed