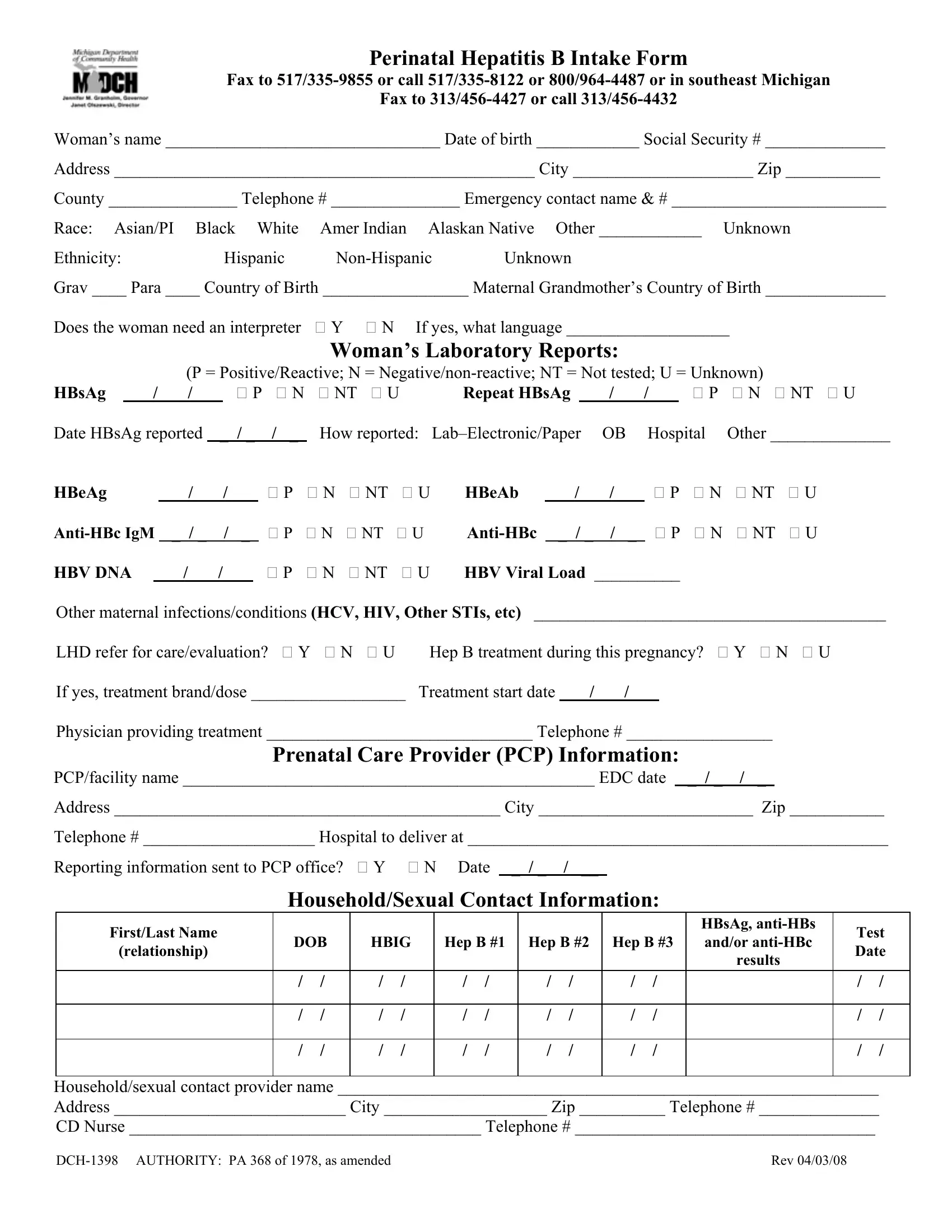
At the intersection of public health and patient care management lies the Perinatal Hepatitis B Intake Form, known formally as the DCH 1398 form. This critical document serves a dual purpose: it is both a reporting tool for healthcare providers and a means to ensure that pregnant women who are carriers of Hepatitis B receive the appropriate follow-up care. The form meticulously collects data ranging from basic demographic information, such as the woman's name, date of birth, and contact details, to more detailed medical history, including Hepatitis B surface antigen (HBsAg) testing results and any need for an interpreter due to language barriers. Furthermore, it delves into the woman's laboratory reports, documenting the presence or absence of various Hepatitis B markers and the viral load, which are crucial for assessing the disease's progression and managing it effectively. The form also captures information regarding the woman's prenatal care provider, the planned hospital for delivery, and any household or sexual contacts that may also be at risk, emphasizing the comprehensive approach towards managing Hepatitis B in a perinatal context. Through its exhaustive data collection, the DCH 1398 form plays an instrumental role in monitoring the spread of Hepatitis B, guiding treatment protocols, and ultimately safeguarding both maternal and neonatal health.
| Question | Answer |
|---|---|
| Form Name | Form Dch 1398 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | _PerinatalHepat itisBIntakeForm 040308_231888_7 hepatitis b vaccine intake form |

Perinatal Hepatitis B Intake Form
Fax to
Fax to
Woman’s name ________________________________ Date of birth ____________ Social Security # ______________
Address _________________________________________________ City _____________________ Zip ___________
County _______________ Telephone # _______________ Emergency contact name & # _________________________
Race: Asian/PI |
Black White |
Amer Indian Alaskan Native Other ____________ Unknown |
|
Ethnicity: |
Hispanic |
Unknown |
|
Grav ____ Para ____ Country of Birth _________________ Maternal Grandmother’s Country of Birth ______________
Does the woman need an interpreter Y N If yes, what language ___________________
Woman’s Laboratory Reports:
|
|
|
(P = Positive/Reactive; N = |
|
|||||||||||||||||||||||
HBsAg _ / _ / _ |
|
|
P |
N |
|
NT U |
Repeat HBsAg |
_ / _ |
|
/ _ |
|
P |
N NT U |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Date HBsAg reported |
|
_ |
/ _ |
|
/ _ |
|
How reported: |
OB |
|
|
Hospital |
Other ______________ |
|||||||||||||||
HBeAg |
_ / _ |
|
/ |
_ |
|
|
P |
N |
NT |
U |
HBeAb |
_ / _ |
/ |
_ |
|
P |
N |
NT |
U |
||||||||
_ / _ |
|
/ |
_ |
|
|
P |
N |
NT |
U |
|
_ |
/ _ |
/ |
_ |
|
P |
N |
NT |
U |
||||||||
HBV DNA |
|
_ / _ |
|
/ |
_ |
|
|
P |
N |
NT |
U |
HBV Viral Load __________ |
|
|
|
||||||||||||
Other maternal infections/conditions (HCV, HIV, Other STIs, etc) _________________________________________
LHD refer for care/evaluation? Y N U |
Hep B treatment during this pregnancy? |
Y |
N U |
||||
If yes, treatment brand/dose __________________ |
Treatment start date _ / _ / _ |
|
|
|
|||
|
|
|
|
|
|||
Physician providing treatment _______________________________ Telephone # _________________ |
|||||||
Prenatal Care Provider (PCP) Information: |
|
|
|
||||
PCP/facility name ________________________________________________ EDC date _ |
/ _ / |
_ |
|
||||
|
|
|
|
|
|
|
|
Address _____________________________________________ City _________________________ Zip ___________
Telephone # ____________________ Hospital to deliver at _________________________________________________
Reporting information sent to PCP office? Y N Date _ / _ / __
Household/Sexual Contact Information:
First/Last Name |
|
|
|
|
|
|
|
|
|
|
HBsAg, |
Test |
||
DOB |
HBIG |
Hep B #1 |
Hep B #2 |
Hep B #3 |
and/or |
|||||||||
(relationship) |
Date |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
results |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
/ |
/ |
/ |
/ |
/ |
/ |
/ |
/ |
/ |
/ |
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
/ |
/ |
/ |
/ |
/ |
/ |
/ |
/ |
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
/ |
/ |
/ |
/ |
/ |
/ |
/ |
/ |
/ |
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Household/sexual contact provider name _______________________________________________________________
Address ___________________________ City ___________________ Zip __________ Telephone # ______________
CD Nurse _________________________________________ Telephone # ___________________________________
Rev 04/03/08 |