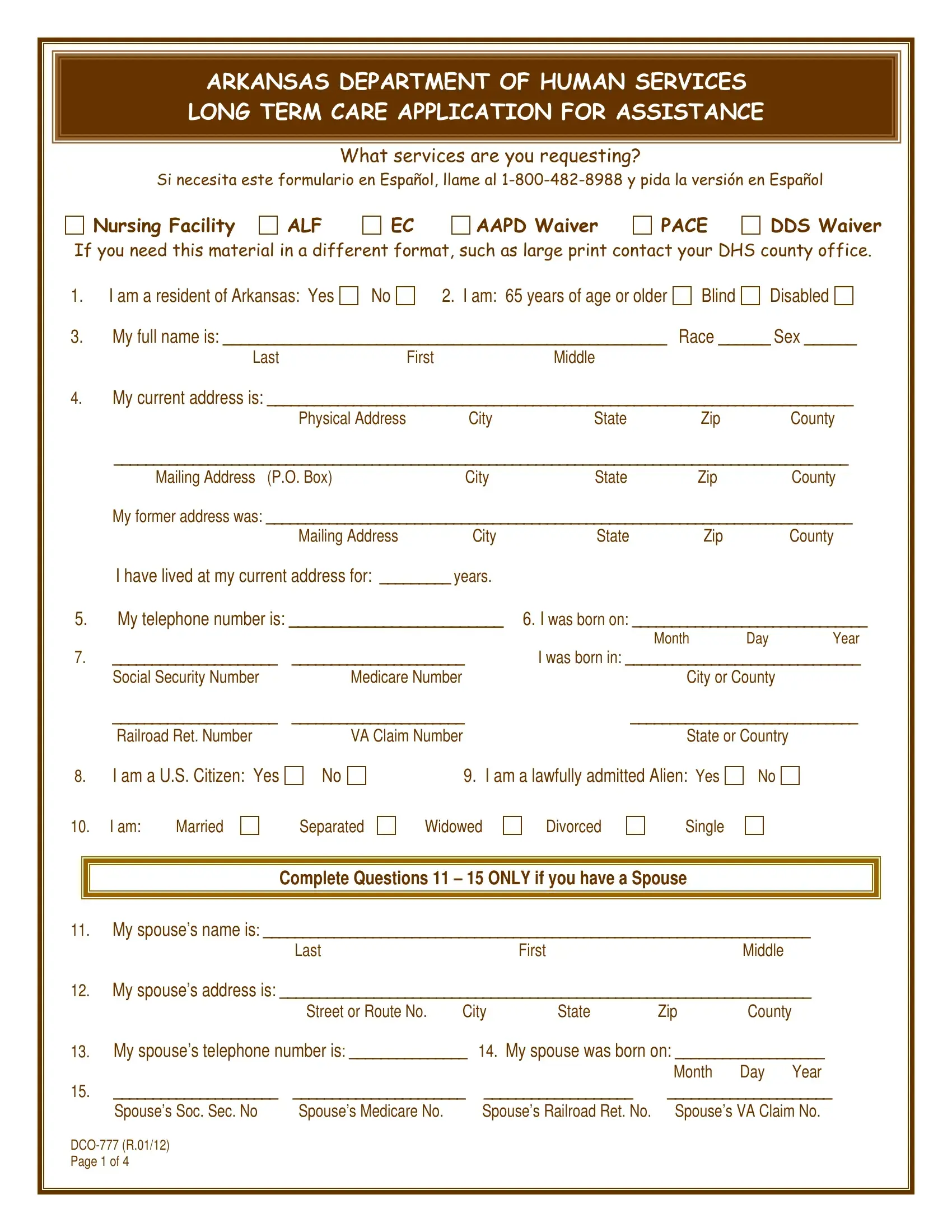
Navigating the complexities of applying for long-term care assistance in Arkansas can be a daunting task, particularly when faced with the multitude of required forms and documentation. Among these, the DCO-777 form plays a critical role, serving as the primary application for those seeking various long-term care services under the auspices of the Arkansas Department of Human Services. This comprehensive document not only requests detailed personal information—ranging from residency and age to marital status and financial background—but also covers a spectrum of care options including Nursing Facility, ALF, EC, AAPD Waiver, PACE, and DDS Waiver services. Importantly, the form is designed with inclusivity in mind, offering translations and alternative formats to accommodate diverse applicants. It meticulously collects data on the applicant and, if applicable, their spouse’s income sources, property ownership, personal belongings of value, and more, to assess eligibility accurately. This process extends to investigating potential changes in the applicant’s financial situation, expectations of income adjustments, and possession or disposal of significant assets. Additionally, the form outlines the importance of understanding Medicaid’s rights to recover costs from an individual’s estate, which may impact decisions on the acceptance and planning of long-term care. The DCO-777 form, therefore, is not merely an application but a crucial step in ensuring that eligible residents of Arkansas receive the care and assistance they need, underscored by a thorough vetting process to determine the most appropriate and financially feasible long-term care solution.
| Question | Answer |
|---|---|
| Form Name | Form Dco 777 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | dco 713 form, dco 777, dhs dco form 777, arkansas form dco 777 |