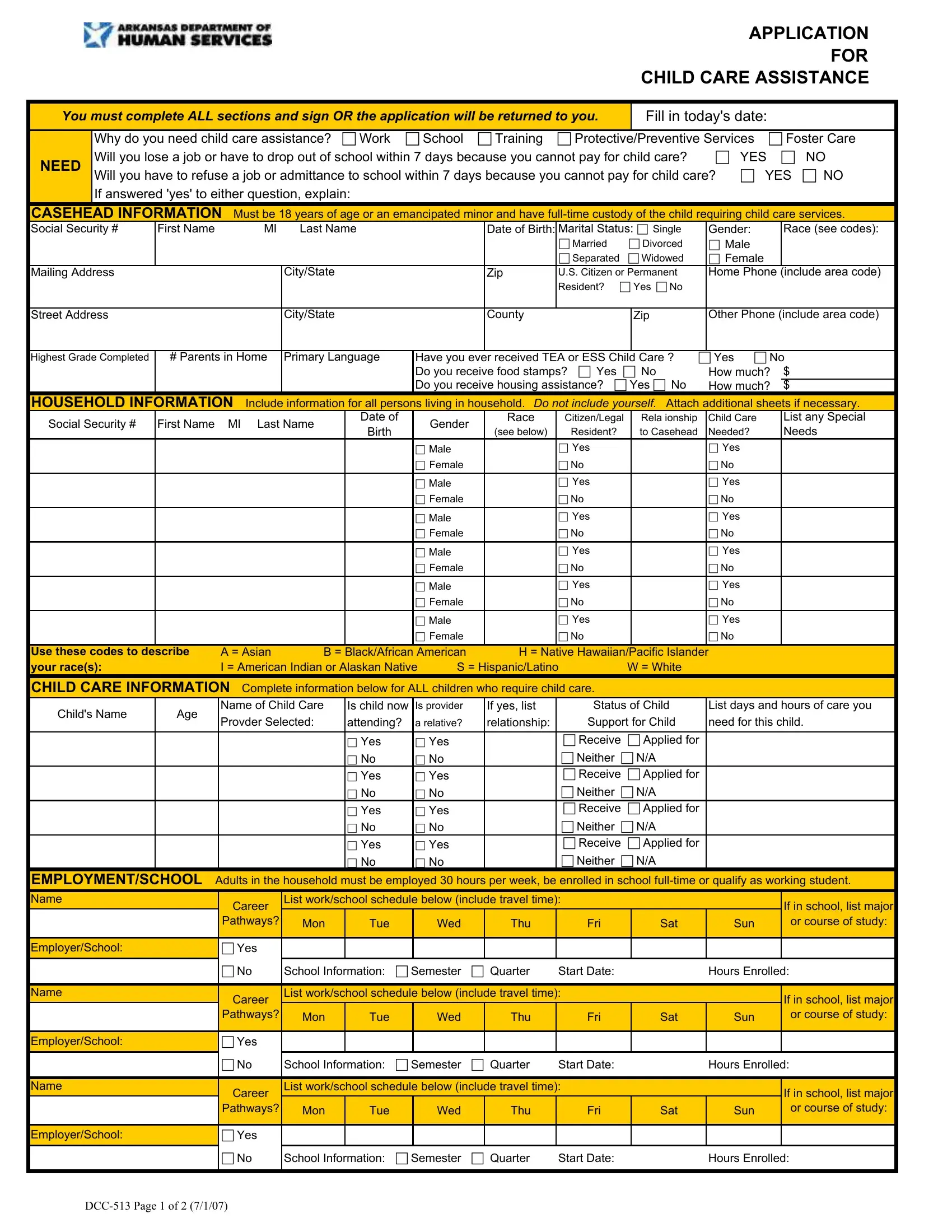
Navigating the process of securing child care assistance can often seem like a daunting task, with various forms and documentation to complete. At the heart of this process for many is the DCO-97 form, an essential application that residents must accurately fill out to potentially qualify for child care assistance. This form is designed to collect comprehensive information about the applicant, including details on the need for child care due to work, school, training, protective/preventive services, or foster care. It emphasizes the urgency of the assistance by asking if the lack of child care could result in job loss or dropping out of school within a specific timeframe. The form further delves into casehead information, household composition, child care specifics, and even the educational or employment details of adults in the household. To be considered, applicants must disclose their financial situation in detail, including income sources and any existing assistance received, such as food stamps or housing aid. Rights and responsibilities are outlined to ensure applicants understand the requirements and obligations associated with applying for and possibly receiving child care assistance. Every section of the DCO-97 form serves a crucial purpose, from establishing eligibility to detailing the care needed for children, making it an indispensable step towards securing necessary support for families in need.
| Question | Answer |
|---|---|
| Form Name | Form Dco 97 |
| Form Length | 6 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 30 sec |
| Other names | arkansas child care assistance form, ar application child care, arkansas child assistance, arkansas child care assistance |