
Dealing with PDF documents online is certainly quite easy using our PDF tool. Anyone can fill out liheap arkansas application here without trouble. Our team is aimed at giving you the perfect experience with our tool by constantly introducing new functions and improvements. With all of these updates, working with our tool gets better than ever! This is what you will want to do to start:
Step 1: Click the orange "Get Form" button above. It is going to open our pdf tool so you could start filling out your form.
Step 2: With this advanced PDF editor, you're able to accomplish more than just complete blank fields. Try all the features and make your docs seem perfect with customized text added, or adjust the original content to excellence - all that comes with the capability to insert stunning images and sign the PDF off.
This document will require specific information to be filled in, therefore you must take the time to fill in precisely what is asked:
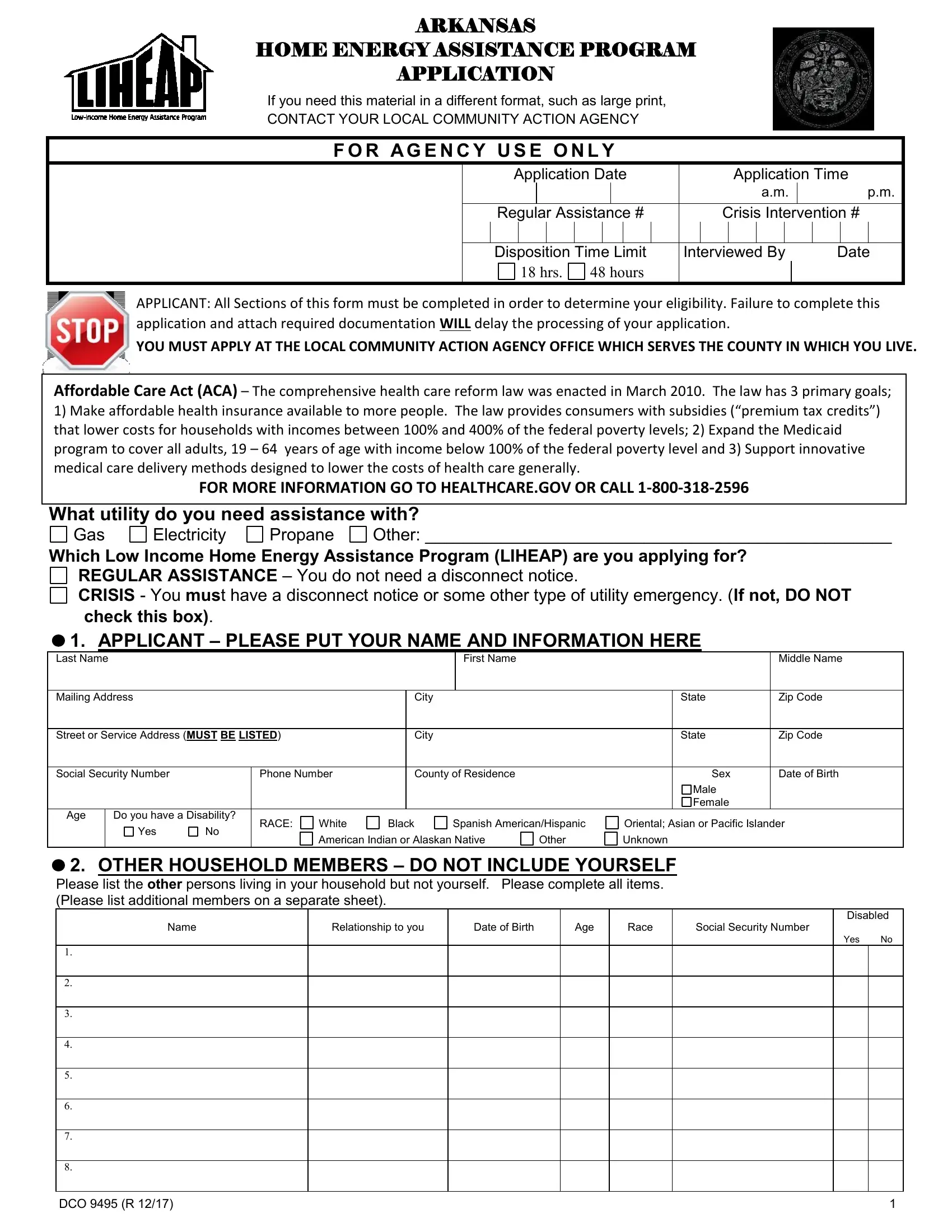
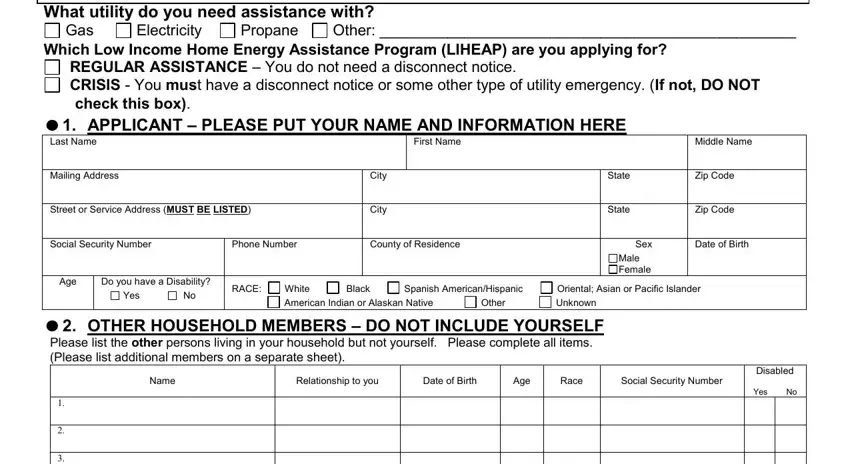
1. It's vital to complete the liheap arkansas application accurately, hence be mindful while working with the sections that contain all of these blank fields:
2. Right after filling out the last step, go on to the subsequent part and fill in the necessary details in all these blanks - DCO R.
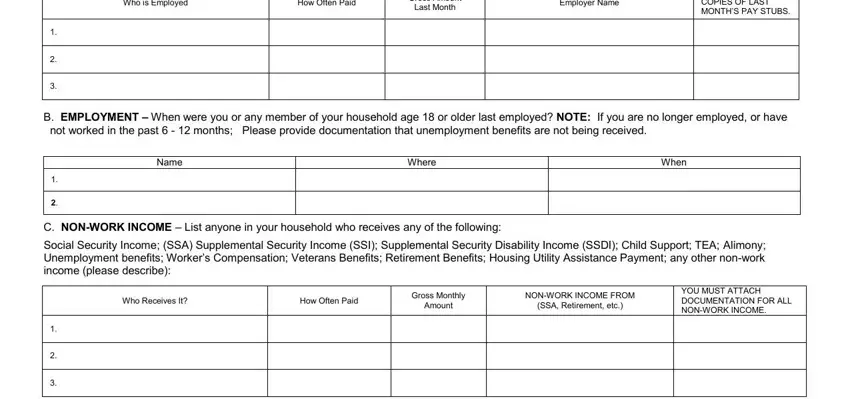
3. The following step is all about Who is Employed, How Often Paid, Gross Amount, Last Month, Employer Name, YOU MUST ATTACH COPIES OF LAST, B EMPLOYMENT When were you or any, Name, Where, When, C NONWORK INCOME List anyone in, Who Receives It, How Often Paid, Gross Monthly, and Amount - fill in every one of these blank fields.
4. To go ahead, this fourth step requires filling in a couple of empty form fields. Examples of these are Resources, Cash on hand, Checking Account, Other Bank Accounts, Other Resources list, YES, Amount, Where, Names of Person, CRISIS APPLICANTS ONLY If your, My home energy utility has been, Electricity, Electricity, Heating, and Heating, which are crucial to carrying on with this document.
5. This pdf should be finished with this particular section. Below you can find a full set of form fields that must be filled in with accurate details for your document submission to be faultless: RENTERS ONLY Is your energy cost, Natural Gas, Electricity, Fuel oil or kerosene, Propane Butane LP or PPG in a, Wood or coal, Other, Check the secondary or other fuel, Natural Gas, Electricity, Fuel oil or kerosene, Propane Butane LP or PPG in a, Wood or coal, Other, and DCO R.

Be really careful while filling out Wood or coal and DCO R, since this is the part in which many people make some mistakes.
Step 3: Soon after proofreading your fields you've filled in, hit "Done" and you are good to go! Download your liheap arkansas application after you sign up for a free trial. Easily view the form inside your personal account page, along with any edits and adjustments all kept! FormsPal is invested in the confidentiality of our users; we always make sure that all personal data processed by our editor remains protected.