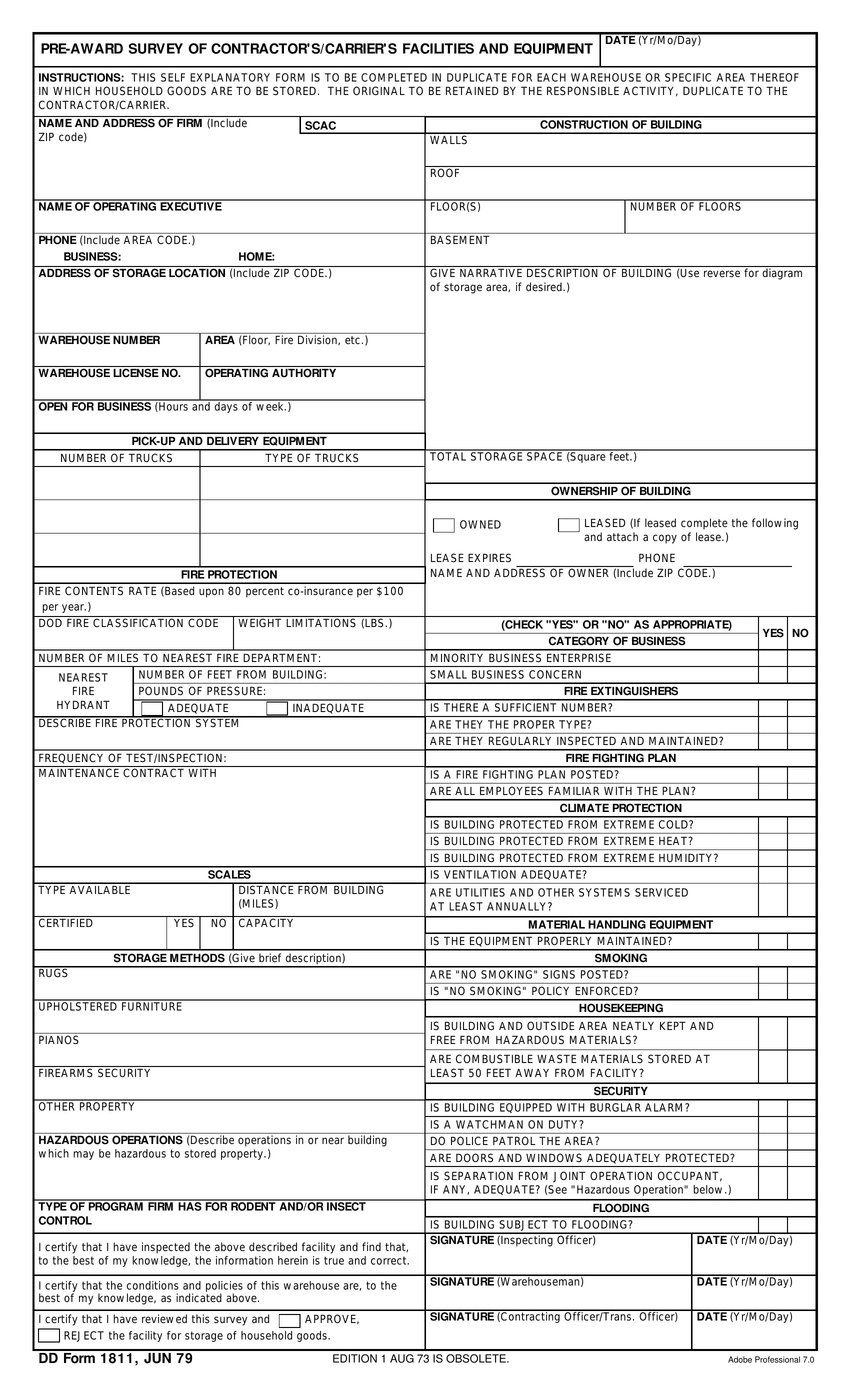
The DD 1811 form, known as the "Pre-Award Survey of Contractor's/Carrier's Facilities and Equipment," plays a crucial role in ensuring the adequacy of facilities where household goods are to be stored prior to a contract award. The form requires comprehensive details about the warehouse or storage area's construction, including the building's walls, roof, floors, and the number of floors. It also dives into specifics such as the operating executive's contact information, storage location, and a narrative description of the building which can include a diagram of the storage area. The form mandates disclosure of the warehouse number, area, warehouse license number, and operating authority, alongside operational details like business hours, pickup and delivery equipment, and total storage space. Additionally, it delves into fire protection measures, climate control, material handling equipment, storage methods, housekeeping standards, security measures against theft or burglary, hazardous operations nearby, and even flooding risks. Contractors or carriers are required to complete this form in duplicate, retaining one copy and submitting the other, ensuring that all information provided is true and correct to the best of their knowledge. This meticulous documentation process is designed to safeguard household goods by establishing strict standards for the facilities where they are stored, reflecting a commitment to security, safety, and operational efficiency.
| Question | Answer |
|---|---|
| Form Name | Form Dd 1811 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | dd form 1811, 1979 form facility equipment, dd 1811 fillable, 1979 dd 1811 contractor |
DATE (Yr/Mo/Day)
INSTRUCTIONS: THIS SELF EXPLANATORY FORM IS TO BE COMPLETED IN DUPLICATE FOR EACH WAREHOUSE OR SPECIFIC AREA THEREOF IN WHICH HOUSEHOLD GOODS ARE TO BE STORED. THE ORIGINAL TO BE RETAINED BY THE RESPONSIBLE ACTIVITY, DUPLICATE TO THE CONTRACTOR/CARRIER.
NAME AND ADDRESS OF FIRM (Include |
SCAC |
|
CONSTRUCTION OF BUILDING |
||
ZIP code) |
|
|
WALLS |
|
|
|
|
|
|
|
|
|
|
|
ROOF |
|
|
|
|
|
|
|
|
NAME OF OPERATING EXECUTIVE |
|
FLOOR(S) |
|
NUMBER OF FLOORS |
|
|
|
|
|
|
|
PHONE (Include AREA CODE.) |
|
|
BASEMENT |
|
|
BUSINESS: |
HOME: |
|
|
|
|
|
|
||||
ADDRESS OF STORAGE LOCATION (Include ZIP CODE.) |
GIVE NARRATIVE DESCRIPTION OF BUILDING (Use reverse for diagram |
||||
|
|
|
of storage area, if desired.) |
||
|
|
|
|
|
|
WAREHOUSE NUMBER |
AREA (Floor, Fire Division, etc.) |
|
|
|
|
|
|
|
|
|
|
WAREHOUSE LICENSE NO. |
OPERATING AUTHORITY |
|
|
|
|
|
|
|
|
|
|
OPEN FOR BUSINESS (Hours and days of w eek.)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
NUMBER OF TRUCKS |
|
TYPE OF TRUCKS |
TOTAL STORAGE SPACE (Square feet .) |
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OWNERSHIP OF BUILDING |
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OWNED |
|
|
LEASED (If leased complete the follow ing |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
and attach a copy of lease.) |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LEASE EXPIRES |
|
|
|
PHONE |
|
|
|
|
|
|||
|
|
|
|
|
|
|
FIRE PROTECTION |
|
|
NAME AND ADDRESS OF OWNER (Include ZIP CODE.) |
||||||||||||||||
|
FIRE CONTENTS RATE (Based upon 80 percent |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
per year.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
DOD FIRE CLASSIFICATION CODE |
WEIGHT LIMITATIONS (LBS.) |
|
|
(CHECK "YES" OR "NO" AS APPROPRIATE) |
YES |
NO |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CATEGORY OF BUSINESS |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
NUMBER OF MILES TO NEAREST FIRE DEPARTMENT: |
MINORITY BUSINESS ENTERPRISE |
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NEAREST |
|
NUMBER OF FEET FROM BUILDING: |
SMALL BUSINESS CONCERN |
|
|
|
|
||||||||||||||||||
|
|
FIRE |
|
POUNDS OF PRESSURE: |
|
|
|
|
|
|
FIRE EXTINGUISHERS |
|
|
|
|
|||||||||||
|
HYDRANT |
|
|
|
|
ADEQUATE |
|
|
|
INADEQUATE |
IS THERE A SUFFICIENT NUMBER? |
|
|
|
|
|||||||||||
|
DESCRIBE FIRE |
PROTECTION SYSTEM |
|
|
ARE THEY THE PROPER TYPE? |
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ARE THEY REGULARLY INSPECTED AND MAINTAINED? |
|
|
|
|||||||||
|
FREQUENCY OF TEST/INSPECTION: |
|
|
|
|
|
|
|
|
|
FIRE FIGHTING PLAN |
|
|
|
|
|||||||||||
|
MAINTENANCE CONTRACT WITH |
|
|
|
|
|
IS A FIRE FIGHTING PLAN POSTED? |
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ARE ALL EMPLOYEES FAMILIAR WITH THE PLAN? |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CLIMATE PROTECTION |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IS BUILDING PROTECTED FROM EXTREME COLD? |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IS BUILDING PROTECTED FROM EXTREME HEAT? |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IS BUILDING PROTECTED FROM EXTREME HUMIDITY? |
|
|
||||||||||
|
|
|
|
|
|
|
|
SCALES |
|
|
IS VENTILATION ADEQUATE? |
|
|
|
|
|||||||||||
|
TYPE AVAILABLE |
DISTANCE FROM BUILDING |
ARE UTILITIES AND OTHER SYSTEMS SERVICED |
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
(MILES) |
|
|
AT LEAST ANNUALLY? |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
CERTIFIED |
|
|
|
|
YES |
NO |
CAPACITY |
|
|
|
MATERIAL HANDLING EQUIPMENT |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IS THE EQUIPMENT PROPERLY MAINTAINED? |
|
|
|
|
||||||||
|
|
|
STORAGE METHODS (Give brief description) |
|
|
|
|
|
SMOKING |
|
|
|
|
|||||||||||||
|
RUGS |
|
|
|
|
|
|
|
|
|
|
|
ARE " NO SMOKING" SIGNS POSTED? |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IS " NO SMOKING" POLICY ENFORCED? |
|
|
|
|
||||||||
|
UPHOLSTERED FURNITURE |
|
|
|
|
|
|
|
|
|
HOUSEKEEPING |
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IS BUILDING AND OUTSIDE AREA NEATLY KEPT AND |
|
|
|
|||||||||
|
PIANOS |
|
|
|
|
|
|
|
|
|
|
|
FREE FROM HAZARDOUS MATERIALS? |
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ARE COMBUSTIBLE WASTE MATERIALS STORED AT |
|
|
|
|||||||||
|
FIREARMS SECURITY |
|
|
|
|
|
LEAST 50 FEET AWAY FROM FACILITY? |
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECURITY |
|
|
|
|
|||
|
OTHER PROPERTY |
|
|
|
|
|
IS BUILDING EQUIPPED WITH BURGLAR ALARM? |
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IS A WATCHMAN ON DUTY? |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
HAZARDOUS OPERATIONS (Describe operations in or near building |
DO POLICE PATROL THE AREA? |
|
|
|
|
||||||||||||||||||||
|
w hich may be hazardous to stored property.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
ARE DOORS AND WINDOWS ADEQUATELY PROTECTED? |
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IS SEPARATION FROM JOINT OPERATION OCCUPANT, |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IF ANY, ADEQUATE? (See " Hazardous Operation" below .) |
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
TYPE OF PROGRAM FIRM HAS FOR RODENT AND/OR INSECT |
|
|
|
|
|
FLOODING |
|
|
|
|
|||||||||||||||
|
CONTROL |
|
|
|
|
|
|
|
|
|
|
|
IS BUILDING SUBJECT TO FLOODING? |
|
|
|
|
|||||||||
|
I certify that I have inspected the above described facility and find that, |
SIGNATURE (Inspecting Officer) |
|
DATE (Yr/Mo/Day) |
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
to the best of my know ledge, the information herein is true and correct . |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
I certify that the conditions and policies of this w arehouse are, to the |
SIGNATURE (Warehouseman) |
|
DATE (Yr/Mo/Day) |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
best of my know ledge, as indicated above. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
I certify that I have review ed this survey and |
|
|
APPROVE, |
SIGNATURE (Contracting Officer/Trans. Officer) |
|
DATE (Yr/Mo/Day) |
|||||||||||||||||||
|
|
|
||||||||||||||||||||||||
|
|
REJECT the facility for storage of household goods. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DD FORM 1811, JUN 79 |
|
|
|
|
EDITION 1 AUG 73 IS OBSOLETE. |
|
|
|
|
|
|
ADOBE PROFESSIONAL 7.0 |
|||||||||||||