
Very few things are easier than creating files using the PDF editor. There isn't much you have to do to manage the CERTIFICATIONS document - just follow these steps in the next order:
Step 1: Click on the button "Get Form Here".
Step 2: After you have entered the editing page CERTIFICATIONS, you'll be able to notice all of the actions available for the document within the upper menu.
In order to fill in the document, enter the information the program will request you to for each of the following segments:
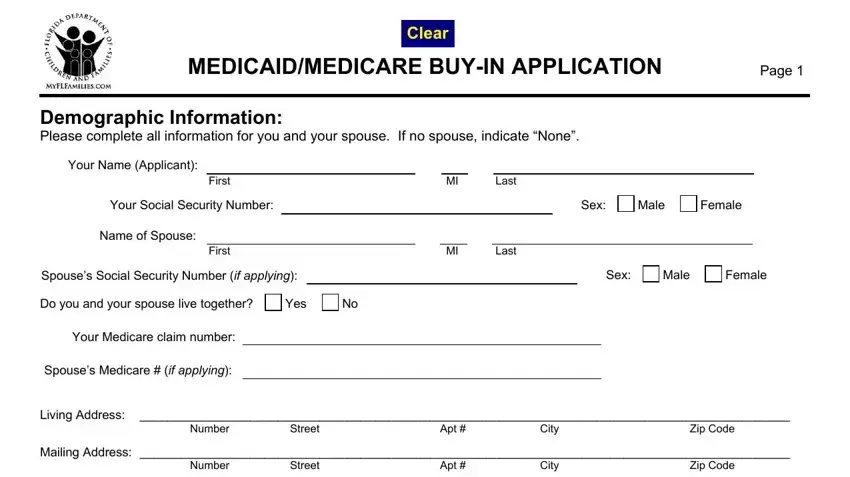
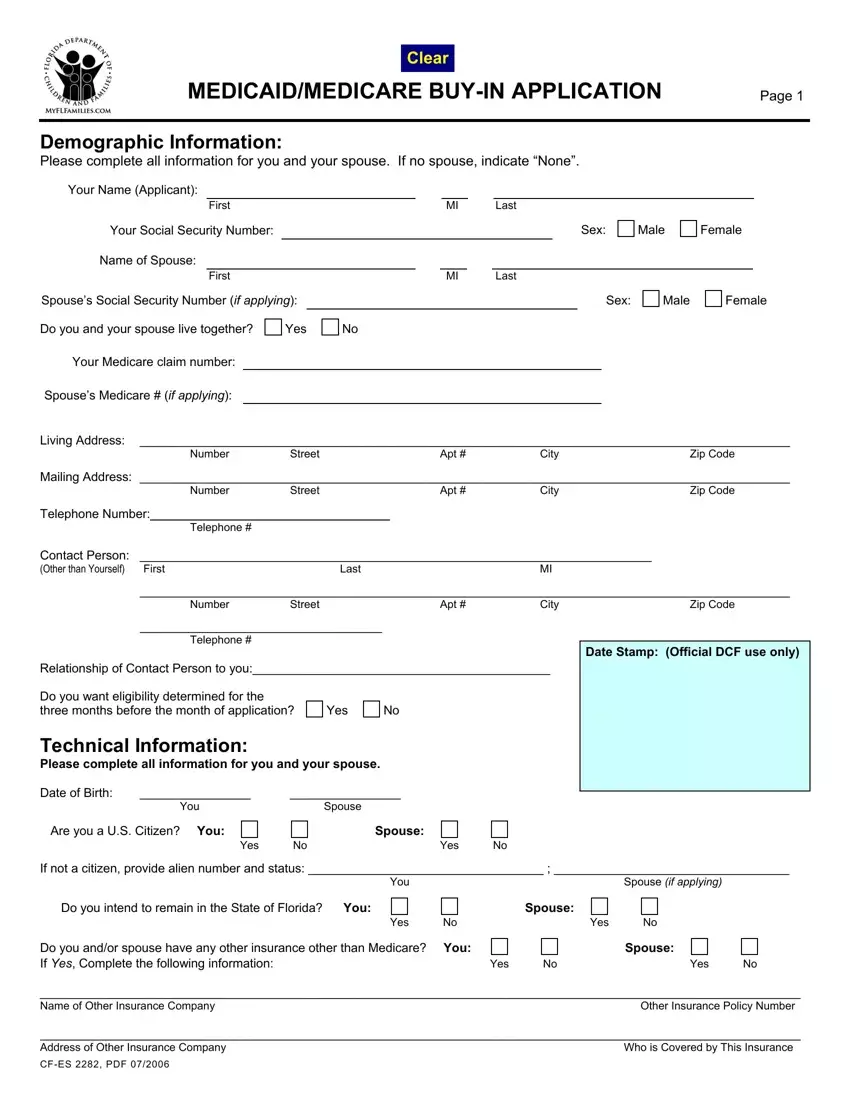
Note the necessary data in the box Telephone, Contact Person Last Other than, Number, Street, Apt, City, Zip Code, Telephone, Relationship of Contact Person to, Date Stamp Official DCF use only, Do you want eligibility determined, Yes, Technical Information Please, Date of Birth, and You.
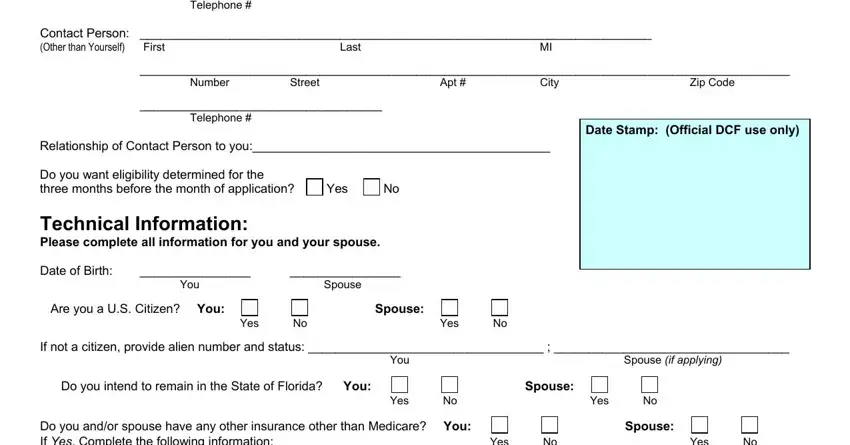
The system will ask you to provide particular significant data to automatically fill in the part Do you andor spouse have any other, Yes, Yes, Name of Other Insurance Company, Address of Other Insurance, and CFES PDF.

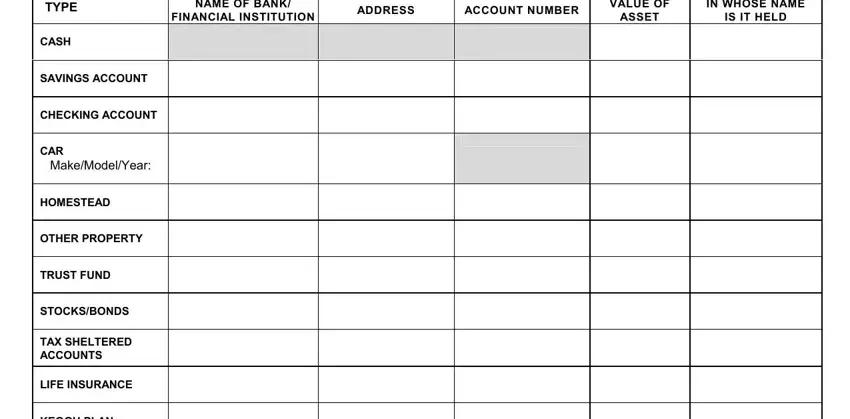
It is important to define the rights and responsibilities of both sides in field NAME OF BANK FINANCIAL INSTITUTION, ADDRESS, ACCOUNT NUMBER, VALUE OF ASSET, IN WHOSE NAME IS IT HELD, TYPE, CASH, SAVINGS ACCOUNT, CHECKING ACCOUNT, CAR, MakeModelYear, HOMESTEAD, OTHER PROPERTY, TRUST FUND, and STOCKSBONDS.
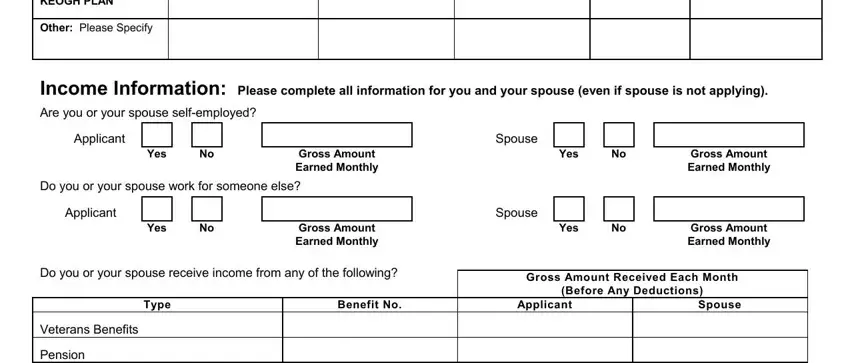
Prepare the document by checking the next sections: KEOGH PLAN, Other Please Specify, Income Information Please complete, Applicant, Yes, Gross Amount Earned Monthly, Yes, Gross Amount Earned Monthly, Spouse, Do you or your spouse work for, Applicant, Yes, Gross Amount Earned Monthly, Yes, and Gross Amount Earned Monthly.
Step 3: When you hit the Done button, your finalized form can be easily exported to any kind of your gadgets or to electronic mail provided by you.
Step 4: Produce a duplicate of each form. It would save you some time and help you avoid complications down the road. Also, your data will not be distributed or viewed by us.
