
Working with PDF forms online is certainly surprisingly easy with this PDF tool. You can fill out Form Dfa 377 4 Qr here within minutes. Our tool is consistently developing to give the very best user experience possible, and that is thanks to our resolve for continual development and listening closely to feedback from users. To begin your journey, go through these simple steps:
Step 1: Just click on the "Get Form Button" at the top of this site to get into our pdf form editor. This way, you'll find all that is necessary to fill out your document.
Step 2: Using this handy PDF editing tool, you can do more than merely fill in blank fields. Express yourself and make your forms seem sublime with custom text added in, or tweak the file's original content to perfection - all comes along with an ability to insert any kind of photos and sign the PDF off.
For you to complete this PDF form, be sure to provide the right details in every area:
1. It is crucial to fill out the Form Dfa 377 4 Qr correctly, so be attentive when working with the areas comprising all these blanks:
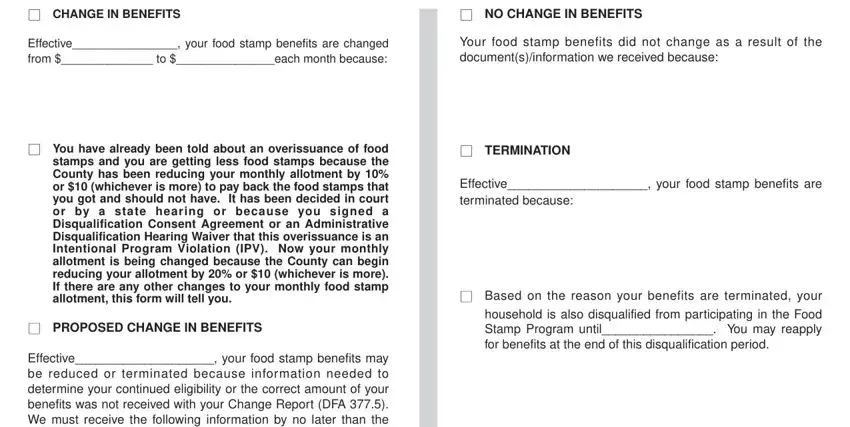
2. Once your current task is complete, take the next step – fill out all of these fields - CHANGE IN BENEFITS, NO CHANGE IN BENEFITS, Effective your food stamp benefits, Your food stamp benefits did not, TERMINATION, Effective your food stamp benefits, Based on the reason your benefits, You have already been told about, PROPOSED CHANGE IN BENEFITS, and Effective your food stamp benefits with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. Completing Effective your food stamp benefits, If verification of an expense is, Rules These rules apply to the, You may review them at your, and DFA QR REQUIRED FORM SUBSTITUTE is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
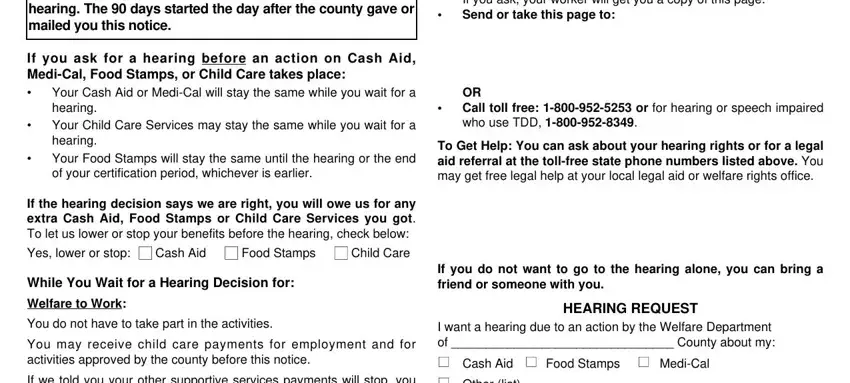
4. It is time to proceed to this fourth portion! In this case you will get all these You have the right to ask for a, If you ask for a hearing before an, Your Cash Aid or MediCal will stay, cid, cid, If the hearing decision says we, Food Stamps, Cash Aid, While You Wait for a Hearing, Welfare to Work, You do not have to take part in, You may receive child care, If we told you your other, cid, and cid blank fields to complete.
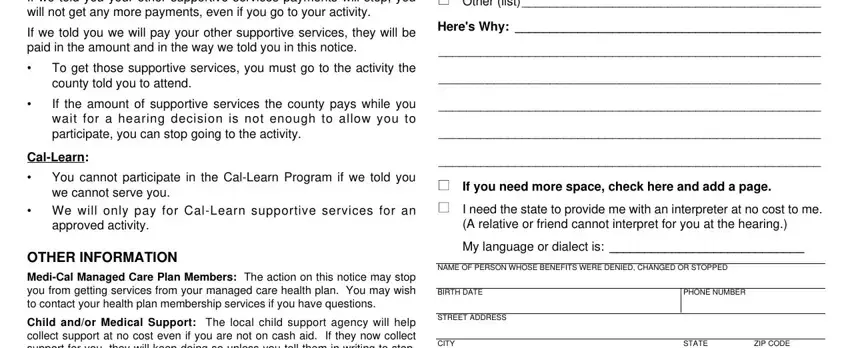
5. Since you approach the finalization of your file, there are actually several more things to complete. Particularly, If we told you your other, If we told you we will pay your, cid, cid, To get those supportive services, If the amount of supportive, CalLearn, cid, You cannot participate in the, cid We will only pay for CalLearn, approved activity, OTHER INFORMATION, MediCal Managed Care Plan Members, Child andor Medical Support The, and I want a hearing due to an action should be filled out.
Be very mindful while filling out cid and approved activity, as this is where many people make errors.
Step 3: Right after you have looked once more at the details provided, click "Done" to finalize your FormsPal process. Join us now and immediately use Form Dfa 377 4 Qr, set for downloading. All adjustments made by you are kept , making it possible to modify the document later on as needed. When using FormsPal, you can easily complete forms without having to get worried about personal data leaks or entries getting distributed. Our protected platform makes sure that your private details are kept safe.