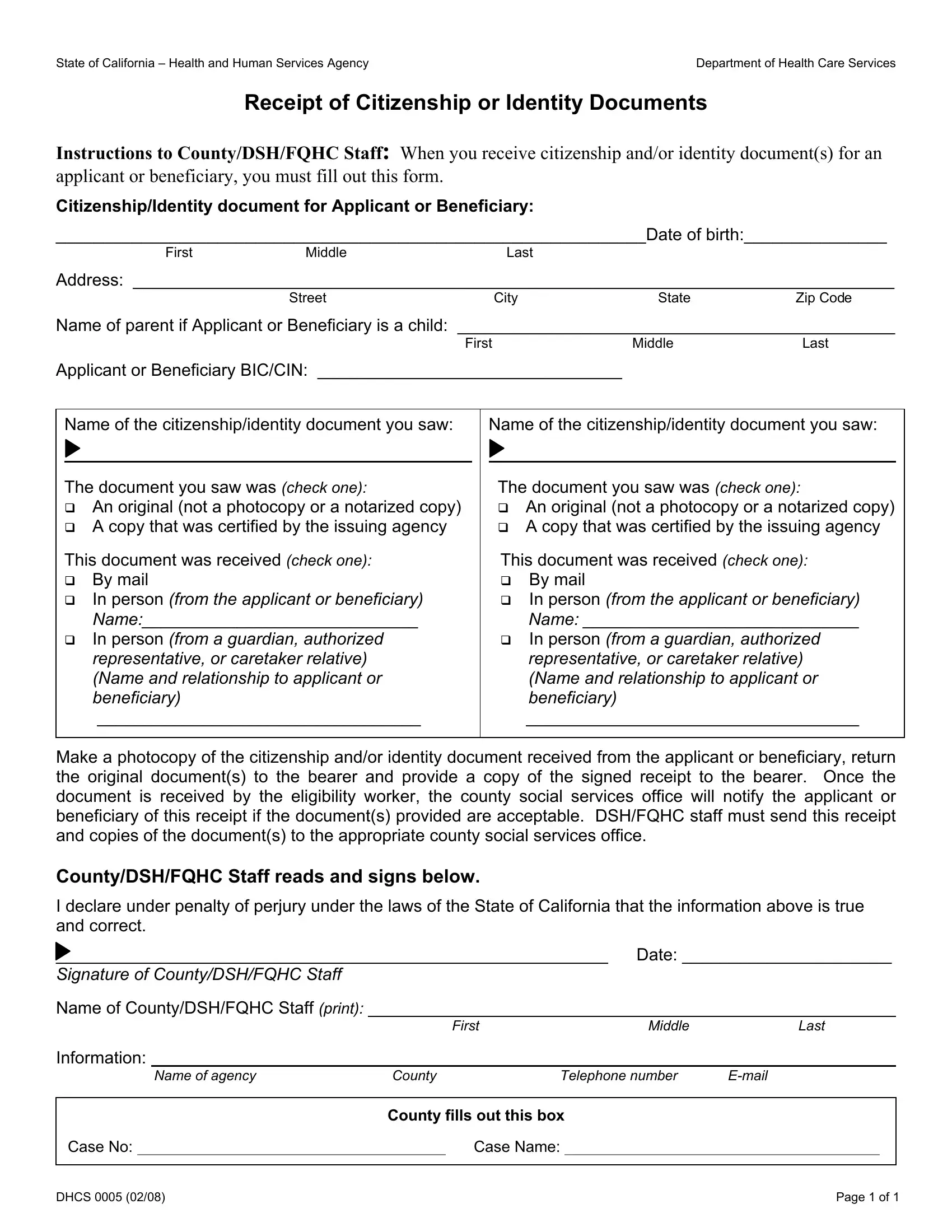
Completing the DHCS 0005 form is a crucial step for anyone applying for health benefits in the State of California, particularly when it comes to verifying citizenship or identity. This form is used by county offices, Department of Social Services (DSH), and Federally Qualified Health Centers (FQHC) staff when they receive crucial documents from applicants or beneficiaries. The purpose of the DHCS 0005 form is multifaceted: it ensures that the necessary documentation for establishing citizenship or identity is formally acknowledged, that the received documentation is either original or a certified copy, and that the details of the document submission process are meticulously recorded. These documents can include, but are not limited to, birth certificates, passports, or state-issued ID cards, depending on what the applicant submits to verify their identity and citizenship. Importantly, this form requires the detailed registration of the document type received, the manner in which it was received (either by mail or in person, and if in person, whether it came directly from the individual or a representative), and the date of receipt. Additionally, the form has provisions for returning the original documents to the submitter, which is crucial for maintaining the applicant's personal document security while also providing a signed receipt as proof of submission. The DHCS 0005 form is designed to maintain transparency and accountability in the eligibility determination process for important health benefits, making it a key component of administrative procedures within California's health and human services framework.
| Question | Answer |
|---|---|
| Form Name | Form Dhcs 0005 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | issuing, dhcs0005, Citizenship, California |
State of California – Health and Human Services Agency |
Department of Health Care Services |
Receipt of Citizenship or Identity Documents
Instructions to County/DSH/FQHC Staff: When you receive citizenship and/or identity document(s) for an applicant or beneficiary, you must fill out this form.
Citizenship/Identity document for Applicant or Beneficiary:
______________________________________________________________Date of birth:_______________
FirstMiddleLast
Address: ________________________________________________________________________________
STREETCityStateZip Code
Name of parent if Applicant or Beneficiary is a child: ______________________________________________
First |
Middle |
Last |
Applicant or Beneficiary BIC/CIN: ________________________________ |
|
|
Name of the citizenship/identity document you saw:
The document you saw was (check one):
An original (not a photocopy or a notarized copy) A copy that was certified by the issuing agency
This document was received (check one): By mail
In person (from the applicant or beneficiary) Name:_____________________________
In person (from a guardian, authorized representative, or caretaker relative) (Name and relationship to applicant or beneficiary)
__________________________________
Name of the citizenship/identity document you saw:
The document you saw was (check one):
An original (not a photocopy or a notarized copy) A copy that was certified by the issuing agency
This document was received (check one): By mail
In person (from the applicant or beneficiary) Name: _____________________________
In person (from a guardian, authorized representative, or caretaker relative) (Name and relationship to applicant or beneficiary)
___________________________________
Make a photocopy of the citizenship and/or identity document received from the applicant or beneficiary, return the original document(s) to the bearer and provide a copy of the signed receipt to the bearer. Once the document is received by the eligibility worker, the county social services office will notify the applicant or beneficiary of this receipt if the document(s) provided are acceptable. DSH/FQHC staff must send this receipt and copies of the document(s) to the appropriate county social services office.
County/DSH/FQHC Staff reads and signs below.
I declare under penalty of perjury under the laws of the State of California that the information above is true and correct.
__________________________________________________________ |
Date: ______________________ |
|||||||
Signature of County/DSH/FQHC Staff |
|
|
|
|
|
|
||
Name of County/DSH/FQHC Staff (print): |
|
|
|
|
|
|
||
|
|
|
|
First |
Middle |
Last |
||
Information: |
|
|
|
|
|
|
||
|
|
Name of agency |
County |
Telephone number |
||||
|
|
|
|
|
|
|
|
|
|
|
|
County fills out this box |
|
|
|
||
Case No: |
|
Case Name: |
|
|
|
|||
|
|
|
|
|
|
|
|
|
DHCS 0005 (02/08) |
Page 1 of 1 |