
Dealing with PDF documents online is very easy using our PDF tool. Anyone can fill out Form Dhcs 4516 here with no trouble. FormsPal team is ceaselessly endeavoring to develop the editor and insure that it is even faster for people with its extensive features. Take your experience to a higher level with continually growing and exceptional possibilities we provide! Here's what you would want to do to start:
Step 1: Simply press the "Get Form Button" in the top section of this page to see our pdf file editor. This way, you'll find everything that is necessary to work with your document.
Step 2: The editor will allow you to work with nearly all PDF files in many different ways. Modify it with personalized text, correct what is already in the document, and place in a signature - all within a few mouse clicks!
This document will need particular data to be typed in, hence be certain to take the time to type in what's expected:
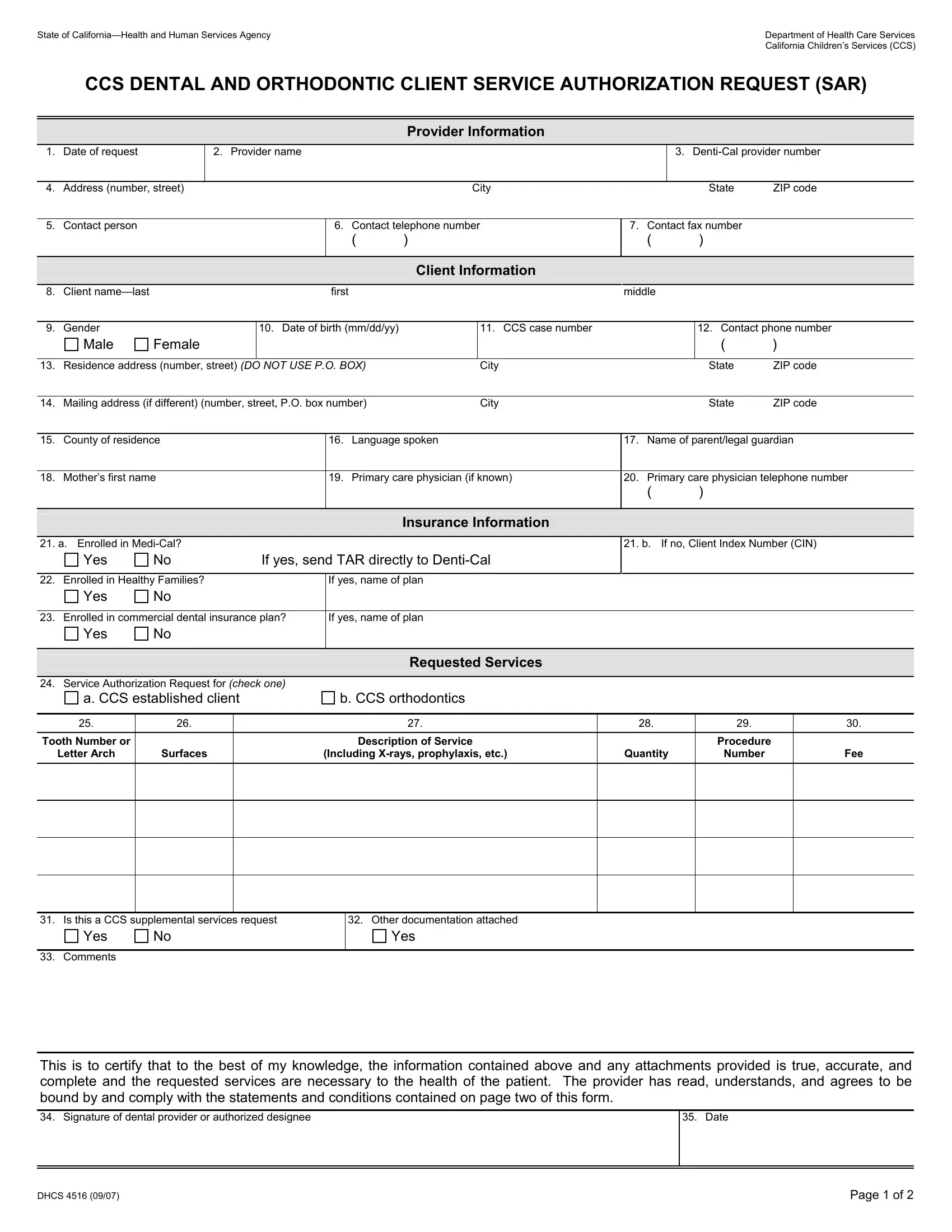
1. First, when filling in the Form Dhcs 4516, beging with the page that contains the following fields:
2. Once this selection of fields is filled out, go to type in the suitable details in all these - Service Authorization Request for, a CCS established client, b CCS orthodontics, Requested Services, Tooth Number or, Letter Arch, Surfaces, Description of Service, Including Xrays prophylaxis etc, Quantity, Procedure, Number, Fee, Is this a CCS supplemental, and Other documentation attached.
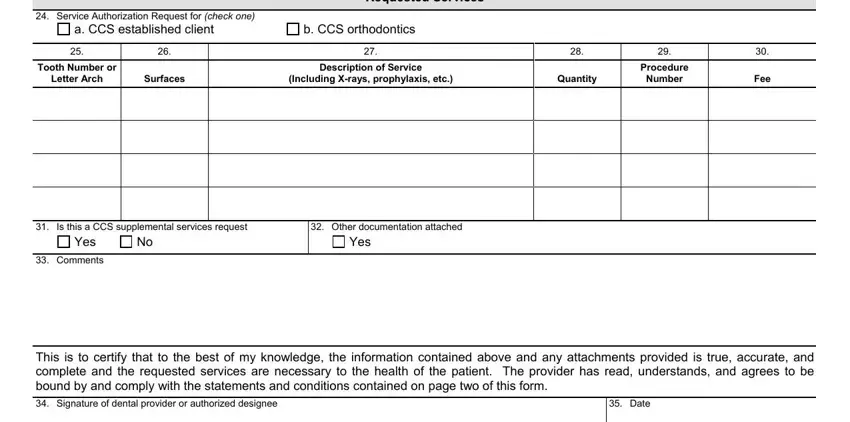
It is possible to make errors while completing the Service Authorization Request for, thus be sure to go through it again before you'll send it in.
Step 3: Right after taking another look at the fields and details, press "Done" and you are all set! Create a free trial option at FormsPal and gain direct access to Form Dhcs 4516 - download, email, or edit from your FormsPal cabinet. Here at FormsPal, we aim to ensure that all your information is kept secure.