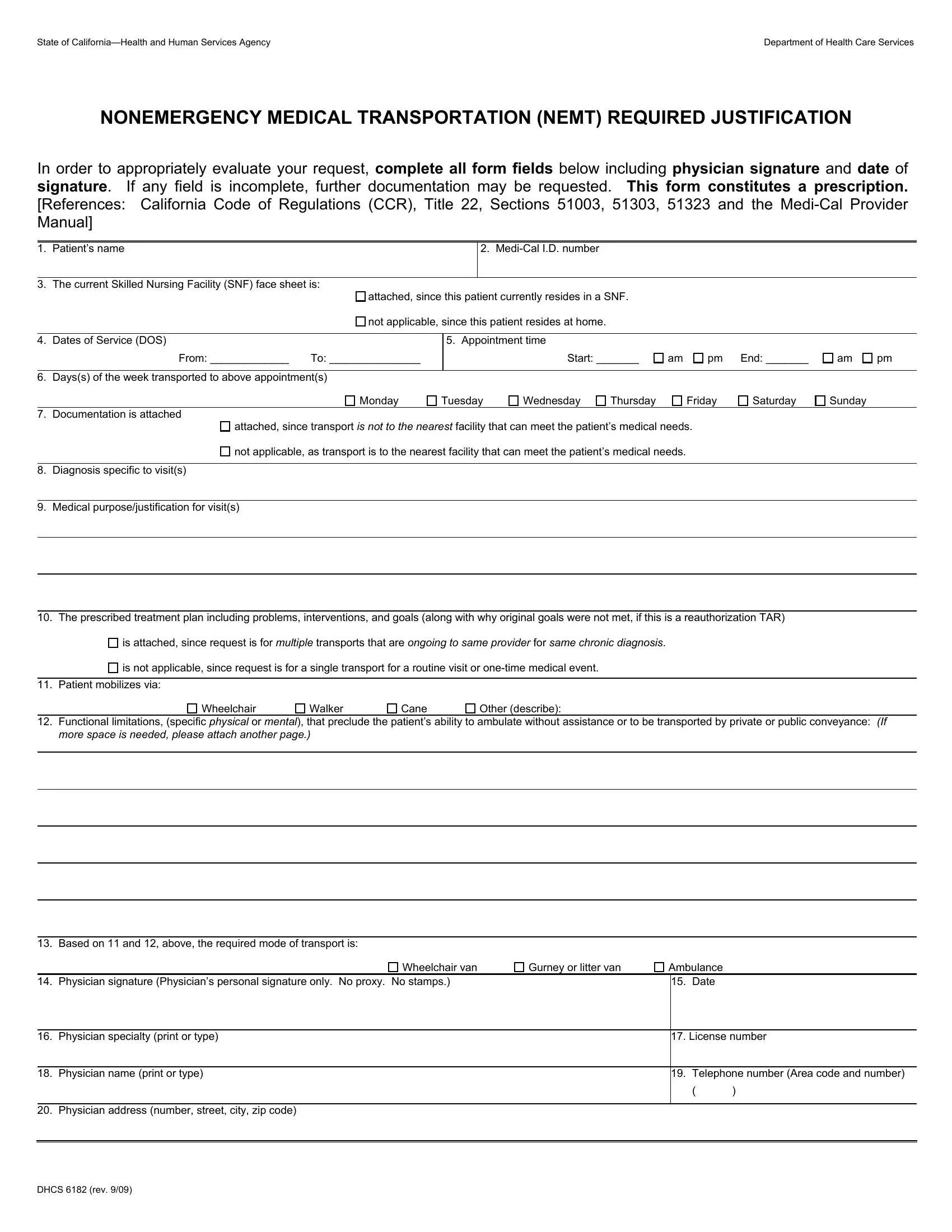
Ensuring access to necessary medical services for individuals with significant mobility challenges is a critical aspect of healthcare management. The State of California—Health and Human Services Agency, through the Department of Health Care Services, provides a systematic approach to facilitate this via the NONEMERGENCY MEDICAL TRANSPORTATION (NEMT) REQUIRED JUSTIFICATION, better known as the DHCS 6182 form. This document serves as a comprehensive tool to justify and authorize the provision of non-emergency medical transport for individuals under the Medi-Cal program. It meticulously captures essential details, starting from the patient’s name and Medi-Cal ID number, through to specifics about the required transport, including the service dates, appointment times, and the patient’s mobility aids, like wheelchairs or canes. Furthermore, critical information regarding the medical necessity for the transportation is detailed, requiring a physician’s diagnosis, the purpose of the medical visit, and a detailed treatment plan including objectives and interventions. Significantly, this form stands as a prescription in itself, necessitating the personal signature of the authorizing physician, thereby ensuring that every nonemergency medical transportation request is backed by a thorough assessment of patient needs, underscoring the form's vital role in patient care coordination.
| Question | Answer |
|---|---|
| Form Name | Form Dhcs 6182 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | dhcs_6182 nemt california form |
