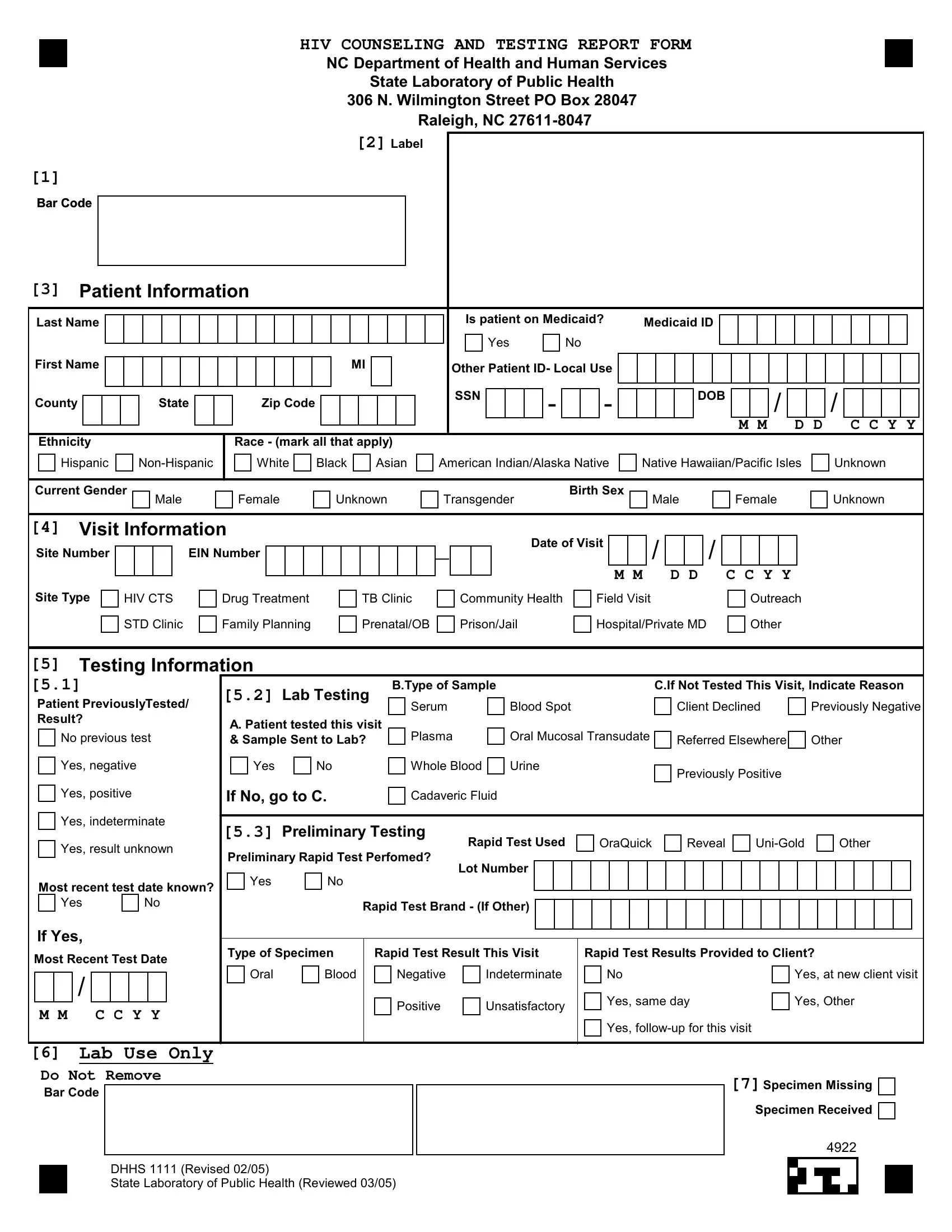
The DHHS 1111 form, integral to the North Carolina Department of Health and Human Services and the State Laboratory of Public Health's efforts to track and manage HIV testing and counseling, embodies a comprehensive tool for gathering critical patient and test information. This form captures a broad spectrum of data starting from basic patient demographics, including name, ethnicity, race, and Medicaid status, to more detailed visit and testing information such as the type and site of visit, reasons for not testing if applicable, and details about any preliminary testing conducted. It also delves into the specifics of lab testing, asking whether the patient was tested during the visit, the type of specimen collected if tested, and the results of any rapid tests conducted. The form is meticulously designed to ensure that patients receive appropriate pre-test counseling, with sections dedicated to capturing whether counseling was provided and if informed consent for testing was obtained. Additionally, it touches on sensitive areas such as pregnancy status in female patients and risk behaviors that might influence an individual's HIV risk profile. By requiring detailed documentation on whether a patient has been previously tested for HIV and the results of those tests, the form plays a crucial role in preventing duplicate testing while ensuring continuity of care. This structured document not only facilitates a systematic approach to HIV counseling and testing but also aids in the collection of vital statistics to monitor and address the HIV/AIDS epidemic in North Carolina.
| Question | Answer |
|---|---|
| Form Name | Form Dhhs 1111 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | HIV_NC_CTR_form state farm consent to rate form |