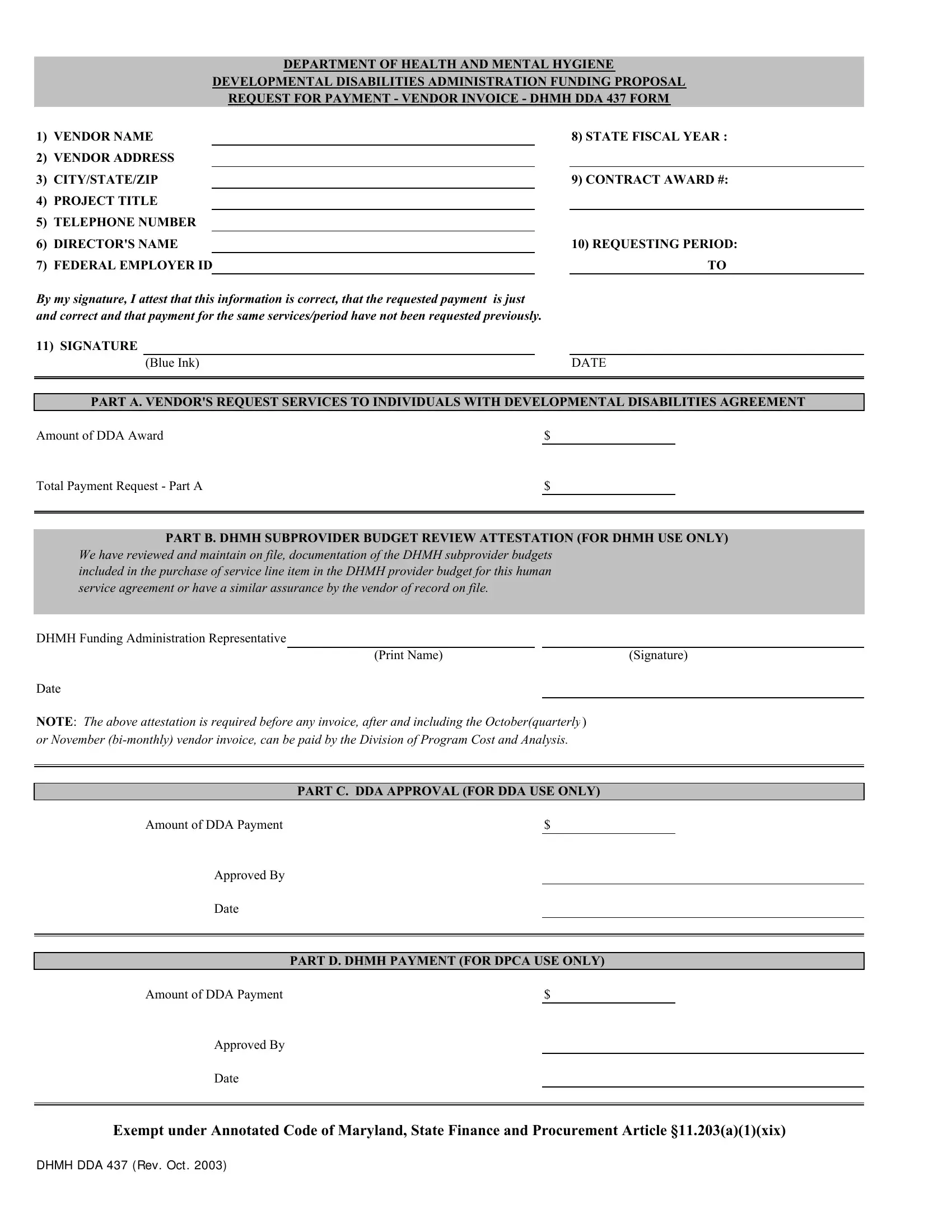
Within the framework of the Department of Health and Mental Hygiene (DHMH), the Developmental Disabilities Administration (DDA) provides critical fiscal support through its Funding Proposal Request for Payment mechanism, encapsulated in the DHMH DDA 437 form. This document serves as a vital tool for vendors seeking reimbursement or payment for services rendered to individuals with developmental disabilities. Detailing essential information such as vendor name, address, project title, and contact details, the form also requires a thorough attestation by the vendor that the payment requested is both just and has not been previously requested for the same services or period. This ensures transparency and accountability in the financial transactions between vendors and the DHMH. Furthermore, it includes sections for the DDA and the DHMH's Division of Program Cost and Analysis (DPCA) to review and approve the requested payment, emphasizing the rigorous oversight in the allocation of funds. With an additional layer of validation through the DHMH subprovider budget review attestation, the process underscores the commitment to judicious financial management in supporting services for individuals with developmental disabilities. This comprehensive approach to funding and payment requests underscores the collaborative effort between various administrative layers to enhance the delivery of services within the sphere of developmental disabilities.
| Question | Answer |
|---|---|
| Form Name | Form Dhmh Dda 437 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | dda437 dhmh 437 form |
DEPARTMENT OF HEALTH AND MENTAL HYGIENE
DEVELOPMENTAL DISABILITIES ADMINISTRATION FUNDING PROPOSAL REQUEST FOR PAYMENT - VENDOR INVOICE - DHMH DDA 437 FORM
1)VENDOR NAME
2)VENDOR ADDRESS
3)CITY/STATE/ZIP
4)PROJECT TITLE
5)TELEPHONE NUMBER
6)DIRECTOR'S NAME
7)FEDERAL EMPLOYER ID
8)STATE FISCAL YEAR :
9)CONTRACT AWARD #:
10)REQUESTING PERIOD: TO
By my signature, I attest that this information is correct, that the requested payment |
is just |
|||
and correct and that payment for the same services/period have not been requested previously. |
||||
11) SIGNATURE |
|
|
|
|
|
(Blue Ink) |
|
|
DATE |
|
|
|
|
|
|
|
|
|
|
PART A. VENDOR'S REQUEST SERVICES TO INDIVIDUALS WITH DEVELOPMENTAL DISABILITIES AGREEMENT
Amount of DDA Award |
$ |
|
Total Payment Request - Part A |
$ |
|
|
|
|
|
|
|
PART B. DHMH SUBPROVIDER BUDGET REVIEW ATTESTATION (FOR DHMH USE ONLY)
We have reviewed and maintain on file, documentation of the DHMH subprovider budgets included in the purchase of service line item in the DHMH provider budget for this human service agreement or have a similar assurance by the vendor of record on file.
DHMH Funding Administration Representative
(Print Name) |
(Signature) |
Date
NOTE: The above attestation is required before any invoice, after and including the October(quarterly ) or November
PART C. DDA APPROVAL (FOR DDA USE ONLY)
Amount of DDA Payment |
$ |
Approved By
Date
PART D. DHMH PAYMENT (FOR DPCA USE ONLY)
Amount of DDA Payment |
$ |
Approved By
Date
Exempt under Annotated Code of Maryland, State Finance and Procurement Article §11.203(a)(1)(xix)
DHMH DDA 437 ( REV. OCT . 2003)