In order to determine a diagnosis, mental health professionals use different diagnostic tools. One of these is the DSM-IV, which is used to diagnose mental disorders. The DSM-IV was last updated in 2000, and so there have been calls for a new revision. Recently, the APA released the draft of the DSM-5, which is set to be released in May 2013. This blog post will discuss some of the changes that have been proposed for the DSM-5. The American Psychiatric Association (APA) has recently released the draft of their upcoming diagnostic manual, the DSM-5. This manual is used by mental health professionals to diagnose mental disorders. There have been a few changes proposed for this edition of the DSM, and we'll take a look at some of them here. One change is that Asperger's Syndrome will be removed and replaced with Autism Spectrum Disorder on both Axis I (clinical disorders) and Axis II (personality disorders). Another change is that Post Traumatic Stress Disorder (PTSD) will now be dia
| Question | Answer |
|---|---|
| Form Name | Form Dhmh Dda 437 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | dda437 dhmh 437 form |
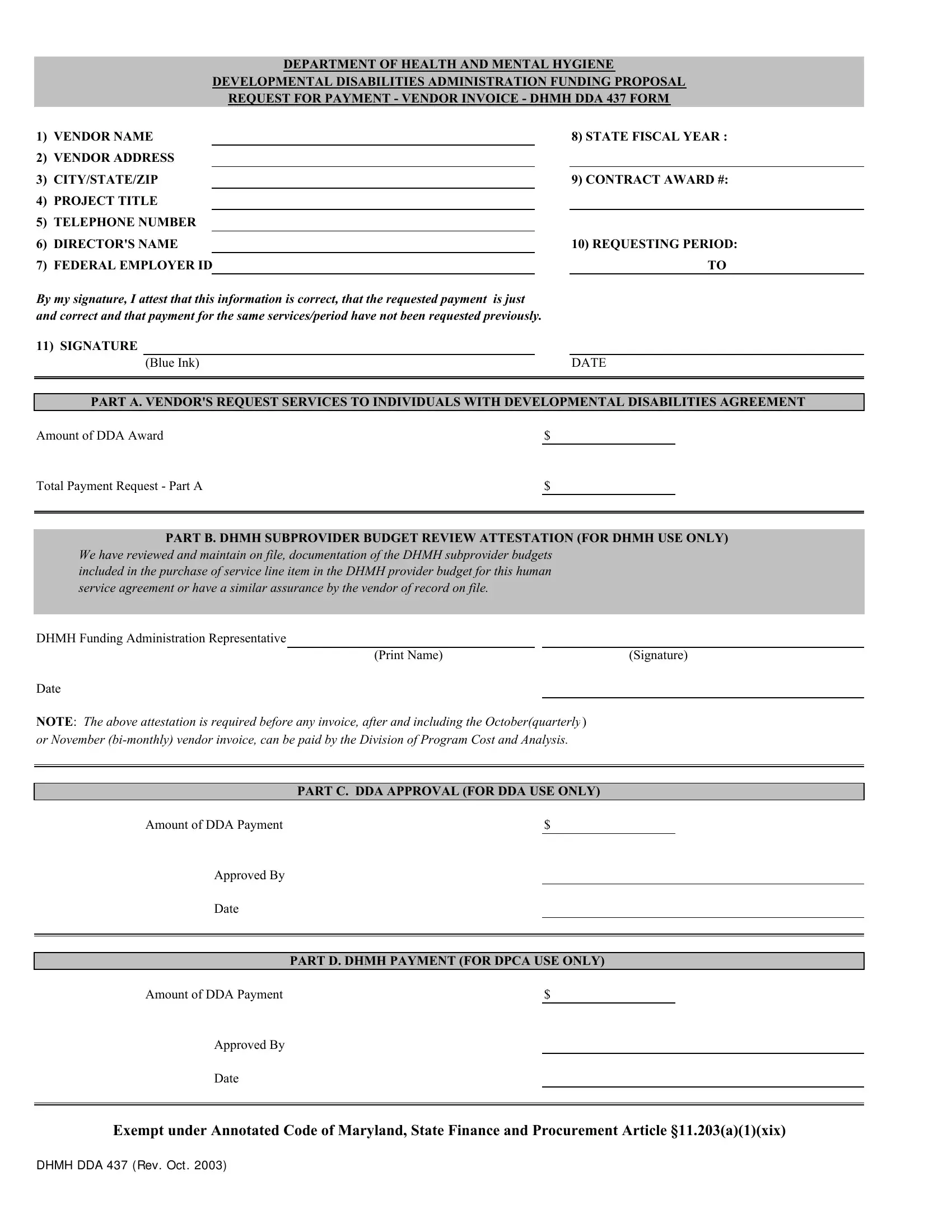
DEPARTMENT OF HEALTH AND MENTAL HYGIENE
DEVELOPMENTAL DISABILITIES ADMINISTRATION FUNDING PROPOSAL REQUEST FOR PAYMENT - VENDOR INVOICE - DHMH DDA 437 FORM
1)VENDOR NAME
2)VENDOR ADDRESS
3)CITY/STATE/ZIP
4)PROJECT TITLE
5)TELEPHONE NUMBER
6)DIRECTOR'S NAME
7)FEDERAL EMPLOYER ID
8)STATE FISCAL YEAR :
9)CONTRACT AWARD #:
10)REQUESTING PERIOD: TO
By my signature, I attest that this information is correct, that the requested payment |
is just |
|||
and correct and that payment for the same services/period have not been requested previously. |
||||
11) SIGNATURE |
|
|
|
|
|
(Blue Ink) |
|
|
DATE |
|
|
|
|
|
|
|
|
|
|
PART A. VENDOR'S REQUEST SERVICES TO INDIVIDUALS WITH DEVELOPMENTAL DISABILITIES AGREEMENT
Amount of DDA Award |
$ |
|
Total Payment Request - Part A |
$ |
|
|
|
|
|
|
|
PART B. DHMH SUBPROVIDER BUDGET REVIEW ATTESTATION (FOR DHMH USE ONLY)
We have reviewed and maintain on file, documentation of the DHMH subprovider budgets included in the purchase of service line item in the DHMH provider budget for this human service agreement or have a similar assurance by the vendor of record on file.
DHMH Funding Administration Representative
(Print Name) |
(Signature) |
Date
NOTE: The above attestation is required before any invoice, after and including the October(quarterly ) or November
PART C. DDA APPROVAL (FOR DDA USE ONLY)
Amount of DDA Payment |
$ |
Approved By
Date
PART D. DHMH PAYMENT (FOR DPCA USE ONLY)
Amount of DDA Payment |
$ |
Approved By
Date
Exempt under Annotated Code of Maryland, State Finance and Procurement Article §11.203(a)(1)(xix)
DHMH DDA 437 ( REV. OCT . 2003)