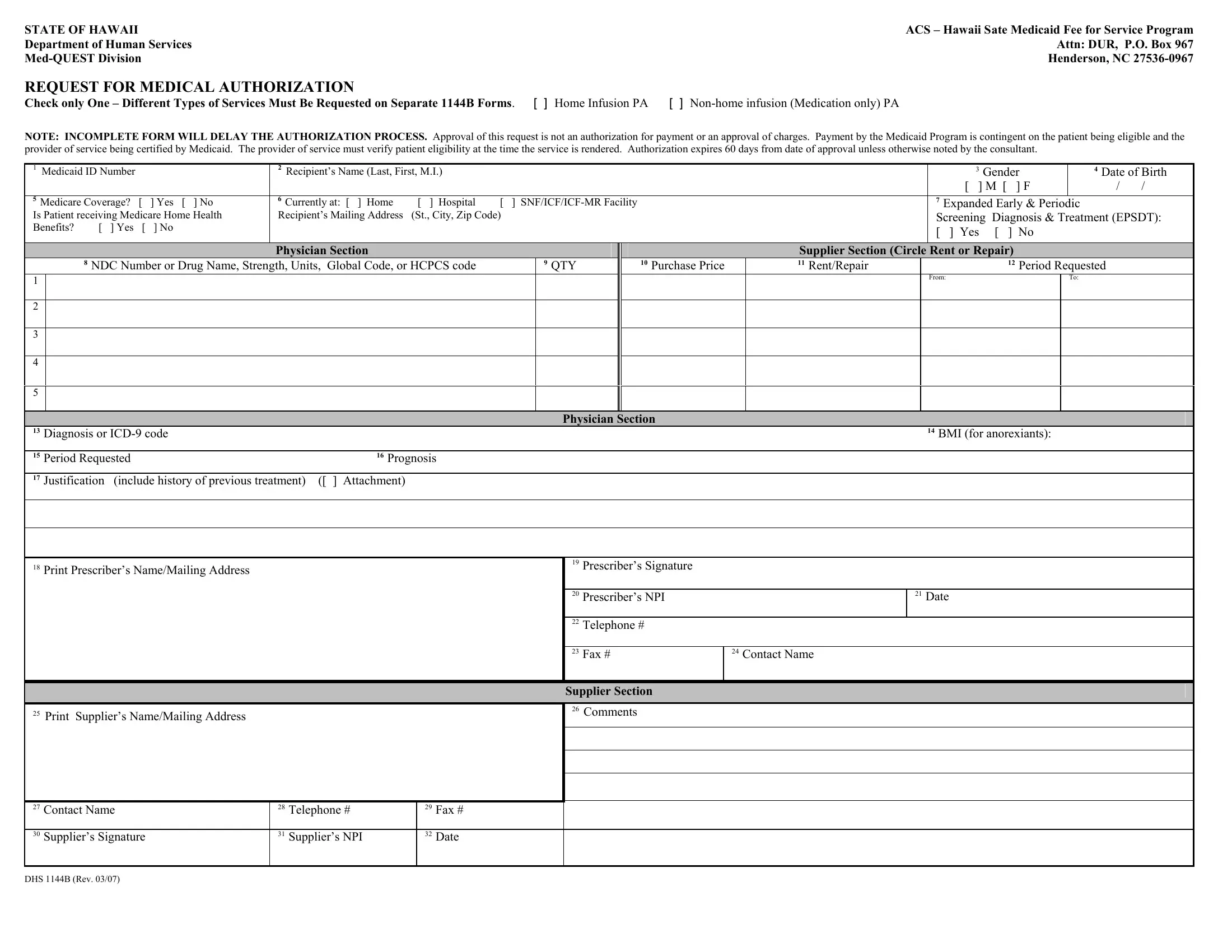
In the intricate landscape of healthcare administration within the United States, particularly in the state of Hawaii, the Dhs 1144B form emerges as a critical document guiding the process of medical authorization under the Med-QUEST Division of the Department of Human Services. This particular form serves as a conduit through which requests for different types of medical services, specifically distinguishing between home infusion and non-home infusion (medication only) Prior Authorization (PA), are meticulously scrutinized and processed. The essence of the form is underscored by its stringent requirement for detailed information, including but not limited to, the Medicaid ID number, recipient's personal information, and specific service requested, thereby ensuring a comprehensive evaluation. Moreover, it highlights the importance of accurate and complete submissions, as any shortcomings directly impact the timely progression of the authorization process. Significantly, the form also delineates the conditional nature of payment approvals, which hinge on the patient's Medicaid eligibility and the provider's certification by Medicaid, emphasizing the need for providers to verify patient eligibility contemporaneously with service delivery. The issuing of authorization, which holds validity for 60 days post-approval, encapsulates a vital procedural step in facilitating access to necessary healthcare services for Medicaid recipients, yet it deliberately clarifies that it does not guarantee payment or endorse the fees charged, preserving the fiscal integrity of the Medicaid program.
| Question | Answer |
|---|---|
| Form Name | Form Dhs 1144B |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | DHS 1144B does california have medquest in sacramento form |
STATE OF HAWAII
Department of Human Services
ACS – Hawaii Sate Medicaid Fee for Service Program Attn: DUR, P.O. Box 967 Henderson, NC
REQUEST FOR MEDICAL AUTHORIZATION
Check only One – Different Types of Services Must Be Requested on Separate 1144B Forms. [ ] Home Infusion PA [ ]
NOTE: INCOMPLETE FORM WILL DELAY THE AUTHORIZATION PROCESS. Approval of this request is not an authorization for payment or an approval of charges. Payment by the Medicaid Program is contingent on the patient being eligible and the provider of service being certified by Medicaid. The provider of service must verify patient eligibility at the time the service is rendered. Authorization expires 60 days from date of approval unless otherwise noted by the consultant.
1 Medicaid ID Number |
|
|
2 Recipient’s Name (Last, First, M.I.) |
|
|
|
|
|
|
|
3 Gender |
|
4 Date of Birth |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
[ ] M [ |
] F |
|
/ |
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
5 Medicare Coverage? |
[ |
] Yes [ ] No |
6 Currently at: [ ] Home |
[ ] Hospital |
[ |
] |
|
|
|
7 Expanded Early & Periodic |
|
|
|||||||
Is Patient receiving Medicare Home Health |
Recipient’s Mailing Address |
(St., City, Zip Code) |
|
|
|
|
|
|
Screening Diagnosis & Treatment (EPSDT): |
||||||||||
Benefits? |
[ ] Yes |
[ |
] No |
|
|
|
|
|
|
|
|
|
[ ] Yes [ |
] No |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
Physician Section |
|
|
|
|
|
|
Supplier Section (Circle Rent or Repair) |
|
|
|||||
|
|
8 NDC Number or Drug Name, Strength, Units, Global Code, or HCPCS code |
|
|
9 QTY |
|
10 Purchase Price |
11 Rent/Repair |
|
12 Period Requested |
|
||||||||
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
From: |
|
|
To: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician Section |
|
|
|
|
|
|
|
|
||
13 Diagnosis or |
|
|
|
|
|
|
|
|
|
14 BMI (for anorexiants): |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
15 Period Requested |
|
|
16 Prognosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
17 Justification (include history of previous treatment) ([ ] Attachment) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
18Print Prescriber’s Name/Mailing Address
19Prescriber’s Signature
20 Prescriber’s NPI |
21 Date |
|
|
22Telephone #
23 Fax # |
24 Contact Name |
|
|
25 Print Supplier’s Name/Mailing Address
Supplier Section
26Comments
27 |
Contact Name |
28 |
Telephone # |
29 |
Fax # |
|
|
|
|
|
|
|
|
30 |
Supplier’s Signature |
31 |
Supplier’s NPI |
32 |
Date |
|
|
|
|
|
|
|
|
DHS 1144B (Rev. 03/07)