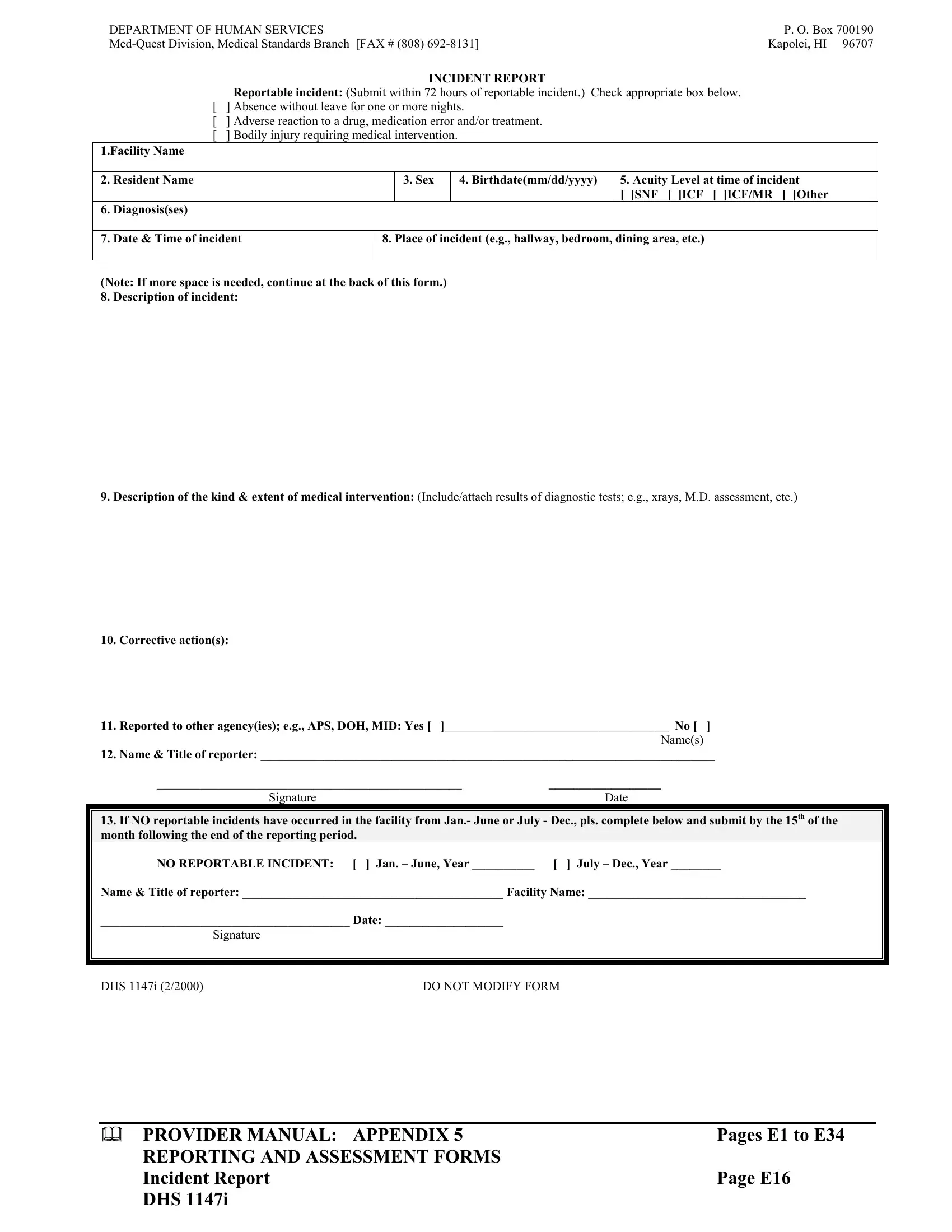
Dealing with incidents in healthcare facilities requires meticulous documentation and prompt reporting, as underscored by forms like the DHS 1147I. This specific form, anchored by the Department of Human Services, plays a pivotal role in ensuring that incidents within such facilities are not only recorded but also addressed with the urgency and seriousness they deserve. Whether it's an adverse reaction to a medication, an error in treatment, absence without leave, or a bodily injury that necessitates medical intervention, this form facilitates a structured approach to reporting. Facilities are mandated to submit detailed reports within 72 hours of the incident, indicating the nature of the event, the individual affected, and the immediate actions taken in response. The documentation extends to the necessary medical interventions that were performed or recommended, underlining the form's comprehensiveness in capturing the incident's impact on the patient's health. Furthermore, it outlines the procedure for facilities to report a period free of incidents, emphasizing a continuous monitoring system. This form thus acts as a crucial tool for the Med-Quest Division, Medical Standards Branch, reinforcing the overarching commitment to maintaining high standards of care and safety in healthcare settings.
| Question | Answer |
|---|---|
| Form Name | Form Dhs 1147I |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Jan, ses, e16 category green card, e16 form |
DEPARTMENT OF HUMAN SERVICES |
P. O. Box 700190 |
Kapolei, HI 96707 |
INCIDENT REPORT
Reportable incident: (Submit within 72 hours of reportable incident.) Check appropriate box below. [ ] Absence without leave for one or more nights.
[] Adverse reaction to a drug, medication error and/or treatment.
[] Bodily injury requiring medical intervention.
1.Facility Name
2. |
Resident Name |
|
3. Sex |
4. Birthdate(mm/dd/yyyy) |
5. Acuity Level at time of incident |
|
|
|
|
|
[ ]SNF [ ]ICF [ ]ICF/MR [ ]Other |
6. |
Diagnosis(ses) |
|
|
|
|
|
|
|
|||
7. |
Date & Time of incident |
8. Place of incident (e.g., hallway, bedroom, dining area, etc.) |
|||
|
|
|
|
||
(Note: If more space is needed, continue at the back of this form.) |
|
|
|||
8. |
Description of incident: |
|
|
|
|
9.Description of the kind & extent of medical intervention: (Include/attach results of diagnostic tests; e.g., xrays, M.D. assessment, etc.)
10.Corrective action(s):
11.Reported to other agency(ies); e.g., APS, DOH, MID: Yes [ ]____________________________________ No [ ] Name(s)
12.Name & Title of reporter: _________________________________________________________________________
_________________________________________________ |
__________________ |
Signature |
Date |
13. If NO reportable incidents have occurred in the facility from Jan.- June or July - Dec., pls. complete below and submit by the 15th of the month following the end of the reporting period.
NO REPORTABLE INCIDENT: [ ] Jan. – June, Year __________ [ ] July – Dec., Year ________
Name & Title of reporter: __________________________________________ Facility Name: ___________________________________
________________________________________ Date: ___________________
|
Signature |
DHS 1147i (2/2000) |
DO NOT MODIFY FORM |
PROVIDER MANUAL: APPENDIX 5 |
Pages E1 to E34 |
REPORTING AND ASSESSMENT FORMS |
|
Incident Report |
Page E16 |
DHS 1147i |
|