
You may prepare household report form effectively in our PDFinity® online PDF tool. To make our tool better and less complicated to use, we continuously come up with new features, taking into account feedback coming from our users. If you're seeking to begin, here is what you will need to do:
Step 1: Hit the orange "Get Form" button above. It is going to open up our editor so that you can start filling in your form.
Step 2: Once you launch the editor, there'll be the form all set to be completed. Apart from filling in different blanks, you may as well perform various other actions with the file, namely writing any text, modifying the original textual content, inserting images, placing your signature to the form, and a lot more.
With regards to the blanks of this particular PDF, this is what you want to do:
1. You need to fill out the household report form correctly, therefore pay close attention while working with the segments including these particular blanks:
2. The subsequent step is to fill in the next few blank fields: Sign and date the form on or after, Return this form no later than, If you need help with the form, If you receive Medical Assistance, Important Read this cid Your, you differently in the handling of, cid How we use this information, and cid Your right to a fair hearing.
Those who use this PDF frequently make errors while completing you differently in the handling of in this part. Be sure to read again everything you type in right here.
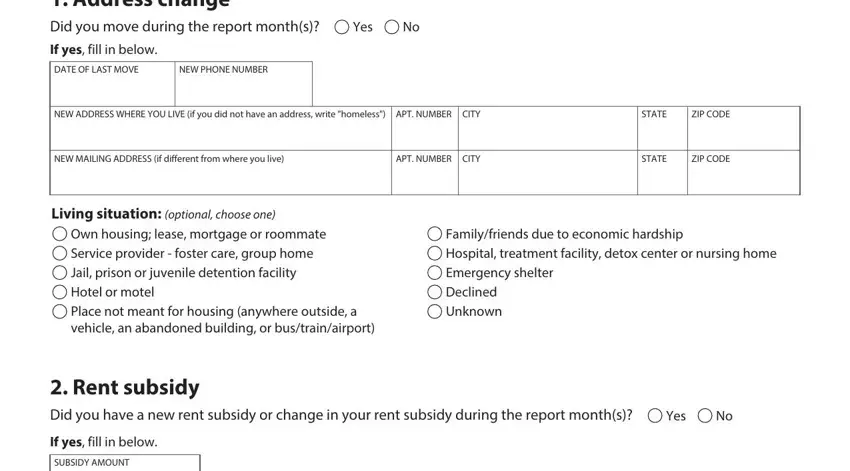
3. This next step is focused on Household Report Form Address, Yes, If yes fill in below, DATE OF LAST MOVE, NEW PHONE NUMBER, NEW ADDRESS WHERE YOU LIVE if you, STATE, ZIP CODE, NEW MAILING ADDRESS if different, APT NUMBER CITY, STATE, ZIP CODE, Living situation optional choose, Own housing lease mortgage or, and Familyfriends due to economic - type in each of these empty form fields.
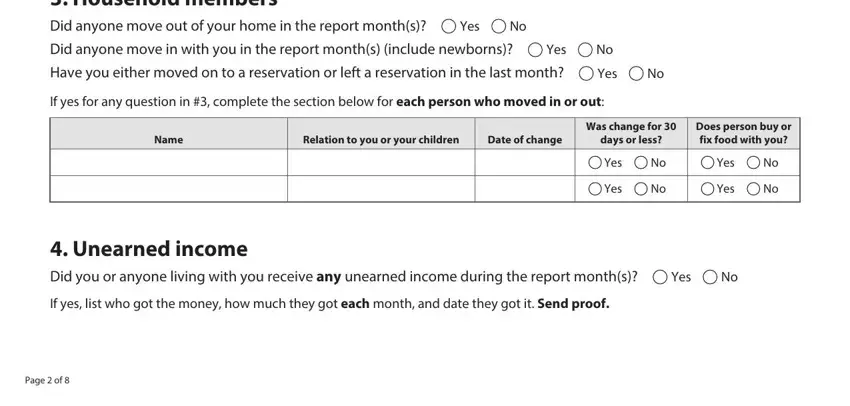
4. All set to begin working on the next form section! Here you have all of these Household members Did anyone move, Yes, Did anyone move in with you in the, Yes, Have you either moved on to a, Yes, If yes for any question in, Name, Relation to you or your children, Date of change, days or less, Was change for, Does person buy or fix food with, Yes, and Yes blanks to do.
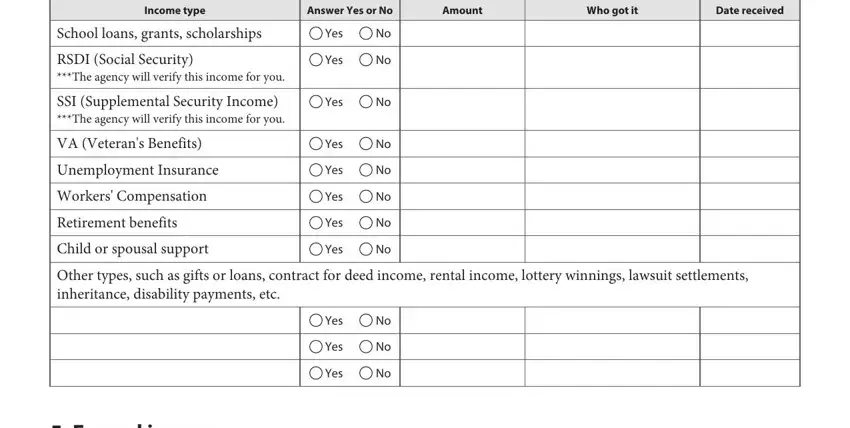
5. Finally, this final section is what you need to wrap up before using the PDF. The blanks at issue are the following: Income type, Answer Yes or No, Amount, Who got it, Date received, School loans grants scholarships, RSDI Social Security The agency, SSI Supplemental Security Income, VA Veterans Benefits, Unemployment Insurance, Workers Compensation, Retirement benefits, Child or spousal support, Yes, and Yes.
Step 3: After you've reread the information you given, click "Done" to conclude your form at FormsPal. Join FormsPal today and immediately obtain household report form, ready for downloading. All modifications made by you are preserved , meaning you can modify the form further as needed. Whenever you work with FormsPal, you can fill out documents without having to be concerned about data incidents or entries being distributed. Our secure system ensures that your private data is maintained safe.