It is easy to fill in the cps 3200 empty lines. Our software can make it virtually effortless to prepare any type of form. Down below are the only four steps you need to consider:
Step 1: To begin, select the orange button "Get Form Now".
Step 2: Now you can modify your cps 3200. You can use the multifunctional toolbar to insert, remove, and adjust the text of the document.
For you to fill in the file, enter the information the software will require you to for each of the next parts:
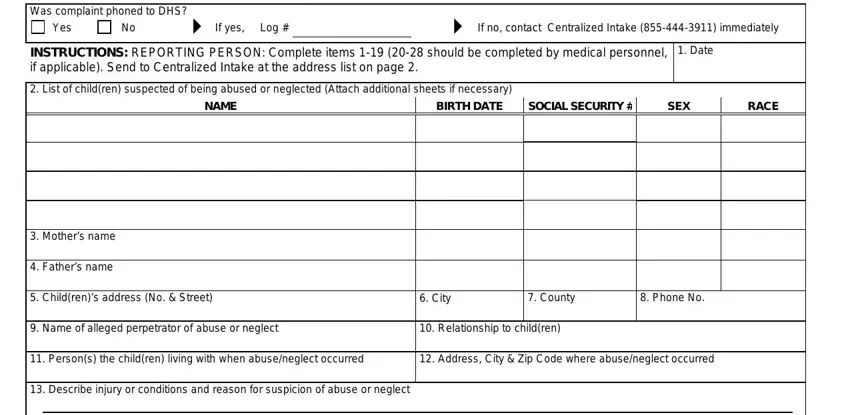
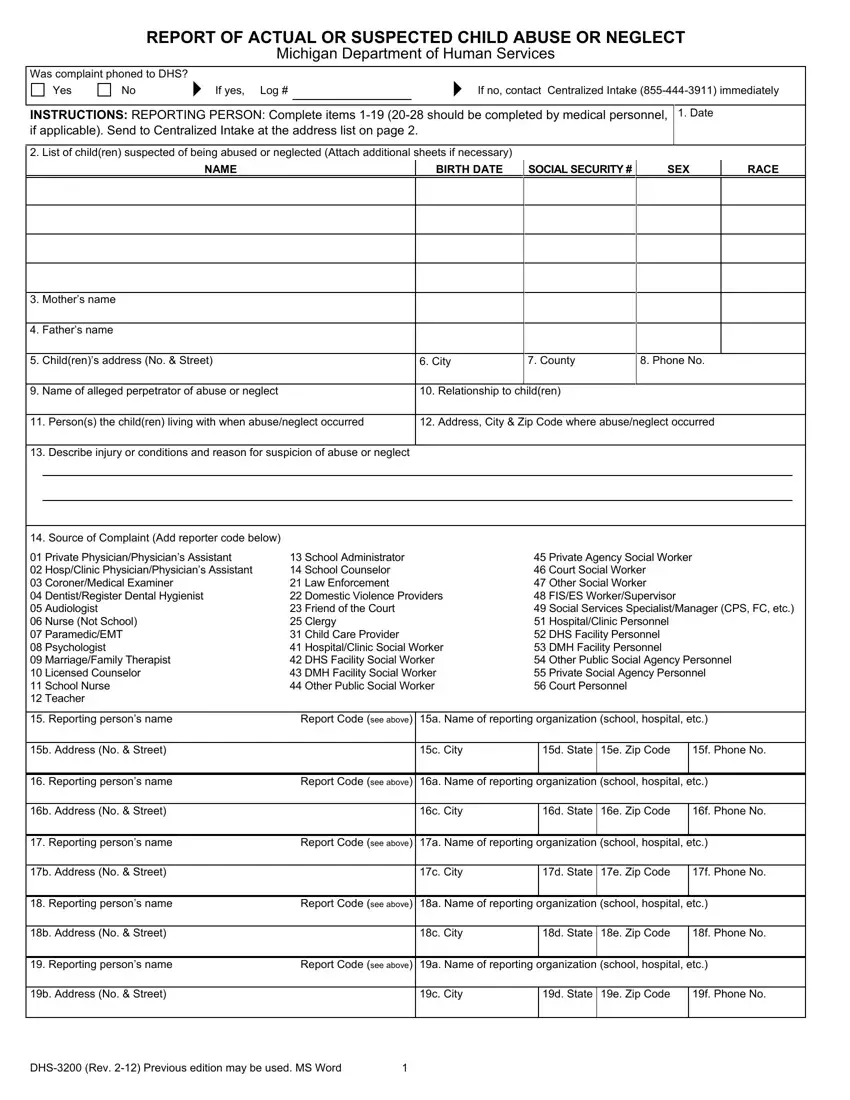
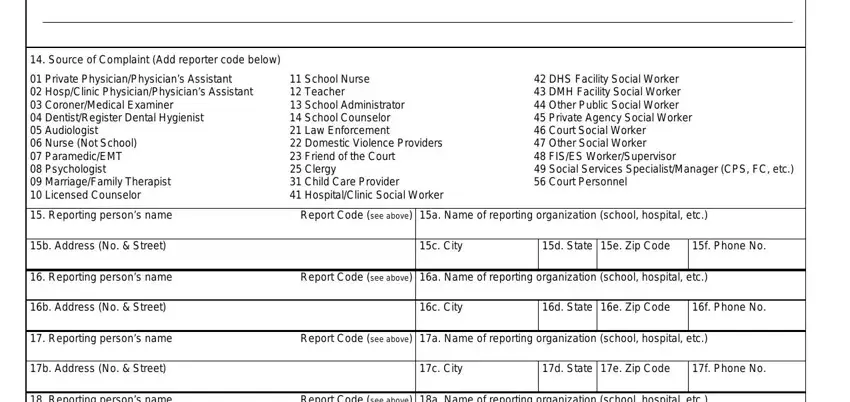
Within the box Source of Complaint Add reporter, Private PhysicianPhysicians, School Nurse Teacher School, DHS Facility Social Worker DMH, Reporting persons name, Report Code see above a Name of, b Address No Street, c City, d State e Zip Code, f Phone No, Reporting persons name, Report Code see above a Name of, b Address No Street, c City, and d State e Zip Code write down the information that the platform asks you to do.
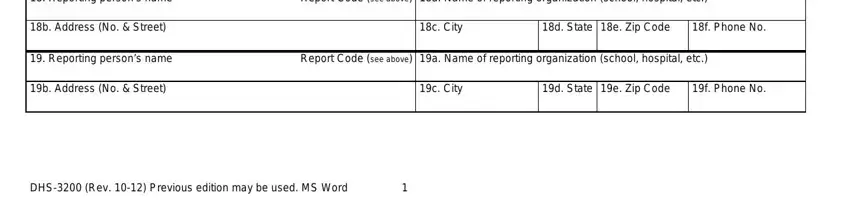
You have to write particular particulars in the space Reporting persons name, Report Code see above a Name of, b Address No Street, c City, d State e Zip Code, f Phone No, Reporting persons name, Report Code see above a Name of, b Address No Street, c City, d State e Zip Code, f Phone No, and DHS Rev Previous edition may be.
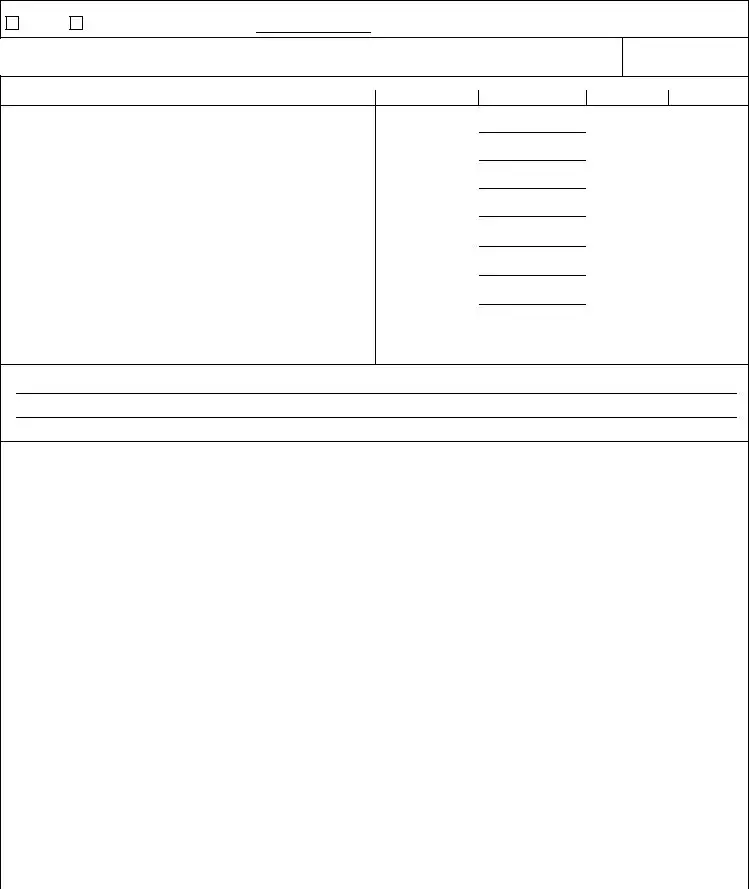
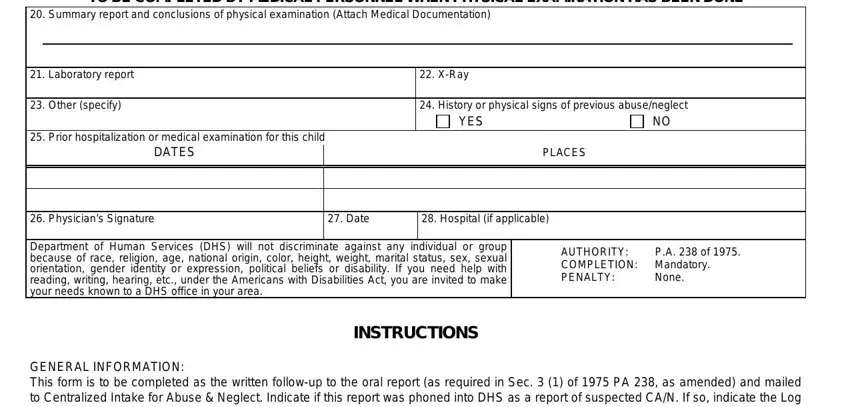
Within the paragraph TO BE COMPLETED BY MEDICAL, Summary report and conclusions of, Laboratory report, Other specify, XRay, History or physical signs of, YES, Prior hospitalization or medical, PLACES, Physicians Signature, Date, Hospital if applicable, Department of Human Services DHS, INSTRUCTIONS, and AUTHORITY COMPLETION Mandatory, write down the rights and obligations of the sides.
Step 3: Hit "Done". You can now upload the PDF document.
Step 4: To prevent any sort of headaches in the foreseeable future, you will need to make at least two or three copies of the file.
