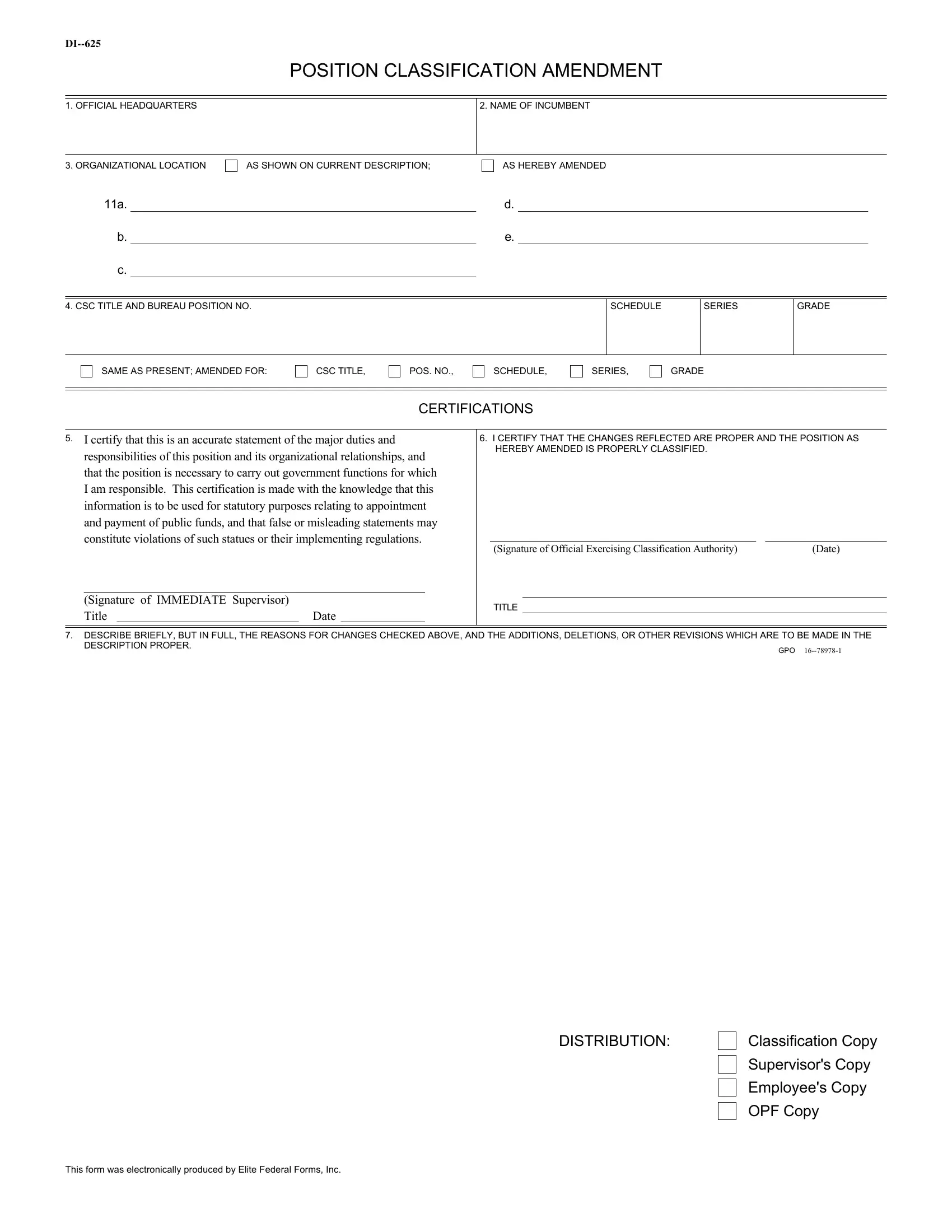
In the realm of government employment, precise classification of positions is crucial to ensure the smooth operation and fairness in the distribution of responsibilities and remunerations. The DI-625 Position Classification Amendment form serves as a vital instrument in this intricate process. It encapsulates official modifications to the classification of a government position, detailing changes in official headquarters, the name of the incumbent, and the organizational location as initially described or as amended. By guiding users through the process of recording modifications in titles, position numbers, schedules, series, and grades, the form maintains the integrity of the position's description and classification. Most importantly, the DI-625 form requires certifications from supervisors and officials exercising classification authority, affirming that the recorded changes are accurate and justified, thereby fulfilling statutory purposes relating to appointment and the allocation of public funds. The final section of the form prompts for a detailed explanation of the reasons behind the noted amendments, enabling a transparent and accountable revision process. Through these meticulously outlined steps, the DI-625 form plays an essential role in upholding the accuracy and legality of government position classifications, reflecting changes that may arise due to organizational restructuring, shifts in responsibilities, or other pertinent factors.
| Question | Answer |
|---|---|
| Form Name | Form Di 625 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | OPF, fillable di 625, form di 625, GPO |
POSITION CLASSIFICATION AMENDMENT
1. OFFICIAL HEADQUARTERS
2. NAME OF INCUMBENT
3. ORGANIZATIONAL LOCATION
AS SHOWN ON CURRENT DESCRIPTION;
AS HEREBY AMENDED
11a.d.
b.e.
c.
4. CSC TITLE AND BUREAU POSITION NO.
SCHEDULE
SERIES
GRADE
SAME AS PRESENT; AMENDED FOR:
CSC TITLE,
POS. NO.,
SCHEDULE,
SERIES,
GRADE
CERTIFICATIONS
5.I certify that this is an accurate statement of the major duties and responsibilities of this position and its organizational relationships, and that the position is necessary to carry out government functions for which I am responsible. This certification is made with the knowledge that this information is to be used for statutory purposes relating to appointment and payment of public funds, and that false or misleading statements may constitute violations of such statues or their implementing regulations.
(Signature of IMMEDIATE Supervisor) |
|
Title |
Date |
6.I CERTIFY THAT THE CHANGES REFLECTED ARE PROPER AND THE POSITION AS HEREBY AMENDED IS PROPERLY CLASSIFIED.
(Signature of Official Exercising Classification Authority) |
(Date) |
TITLE
7. DESCRIBE BRIEFLY, BUT IN FULL, THE REASONS FOR CHANGES CHECKED ABOVE, AND THE ADDITIONS, DELETIONS, OR OTHER REVISIONS WHICH ARE TO BE MADE IN THE
DESCRIPTION PROPER.
GPO
DISTRIBUTION:
Classification Copy
Supervisor's Copy
Employee's Copy
OPF Copy
This form was electronically produced by Elite Federal Forms, Inc.