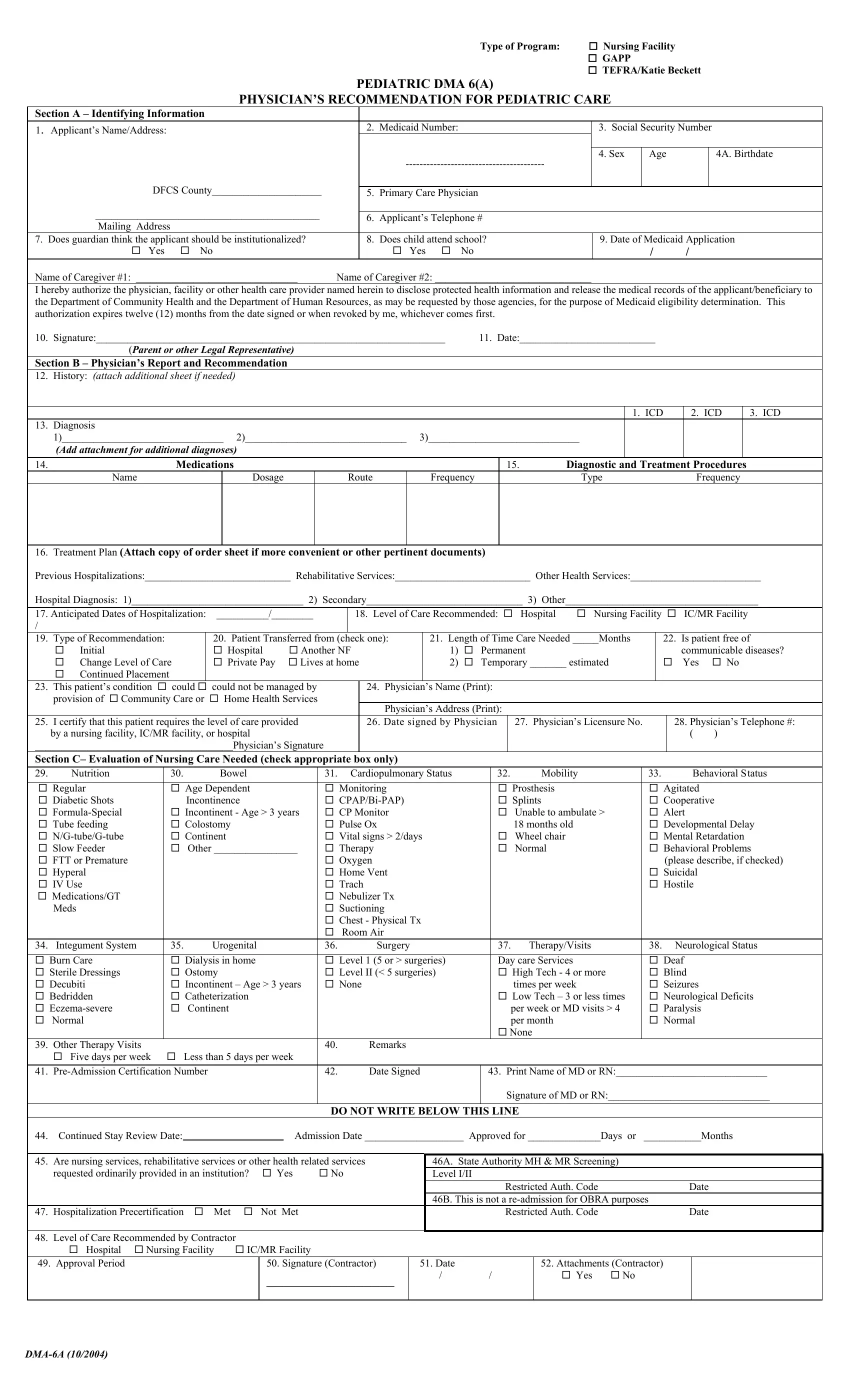
In addition to basic medical information, families and providers often use the DMA 6A form for the TEFRA/Katie Beckett program. It helps show that a child meets an institutional level of care while continuing to live at home. That distinction matters because TEFRA looks at medical need, not family income.
Physicians use the DMA 6A to explain how much care a child needs each day, what type of skilled support is required, and what could happen if services stop.
The DMA-6A form asks the physician to describe the child’s real-life care needs. Doctors explain whether the child needs hands-on nursing care, constant supervision, medical equipment, or frequent treatments. Medicaid reviewers read these details closely to understand how the child functions outside a hospital or facility. Families often submit the Pediatric DMA 6(A) form for new TEFRA applications, renewals, or when a child’s condition changes.
The DMA 6A form commonly covers:
• Level of medical supervision the child needs,
• Skilled nursing tasks and how often they occur,
• Dependence on caregivers for daily activities,
• Medications, therapies, and equipment in use,
• Risk of hospitalization or placement in a facility.
Note! The DMA 6A form is often confused with the Georgia DMA 6 form. DMA 6 applies to adults and nursing facility placement, while DMA 6A is only for children and supports pediatric Medicaid programs like TEFRA.
| Question | Answer |
|---|---|
| Form Name | Form DMA 6A Georgia |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 155 |
| Avg. time to fill out | 20 min |
| Other names | dma-6a form, pediatric dma 6(a) form, Georgia dma 6a, physician recommendation for pediatric care form |
|
|
|
|
|
|
Type of Program: |
Nursing Facility |
|
|
|
|
|
|
|
|
|
|
GAPP |
|
|
|
|
|
|
|
|
|
|
TEFRA/Katie Beckett |
|||
|
|
|
PEDIATRIC DMA 6(A) |
|
|
|
|
|||
|
|
PHYSICIAN’S RECOMMENDATION FOR PEDIATRIC CARE |
|
|
|
|||||
Section A – Identifying Information |
|
|
|
|
|
|
|
|
||
1. |
Applicant’s Name/Address: |
|
|
2. |
Medicaid Number: |
|
3. Social Security Number |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. Sex |
Age |
|
4A. Birthdate |
|
|
|
|
|
|
|
|
|
||
|
DFCS County_____________________ |
|
|
|
|
|
|
|
|
|
|
|
5. |
Primary Care Physician |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|||
|
___________________________________________ |
|
|
|
|
|
|
|
|
|
|
|
6. |
Applicant’s Telephone # |
|
|
|
|
|||
|
Mailing Address |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
7. |
Does guardian think the applicant should be institutionalized? |
|
8. |
Does child attend school? |
9. Date of Medicaid Application |
|||||
|
Yes |
No |
|
|
Yes |
No |
|
/ |
/ |
|
Name of Caregiver #1: _______________________________ |
Name of Caregiver #2: ______________________________ |
|
|
|
|
|||||
I hereby authorize the physician, facility or other health care provider named herein to disclose protected health information and release the medical records of the applicant/beneficiary to the Department of Community Health and the Department of Human Resources, as may be requested by those agencies, for the purpose of Medicaid eligibility determination. This authorization expires twelve (12) months from the date signed or when revoked by me, whichever comes first.
10. Signature:___________________________________________________________________ |
11. Date:__________________________ |
(Parent or other Legal Representative) |
|
Section B – Physician’s Report and Recommendation
12. |
History: (ATTACH ADDITIONAL SHEET IF NEEDED) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. ICD |
|
|
2. ICD |
|
3. ICD |
||||
13. |
Diagnosis |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1)_______________________________ 2)_______________________________ 3)_____________________________ |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
(Add attachment for additional diagnoses) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
14. |
|
|
|
|
Medications |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15. |
|
Diagnostic and Treatment Procedures |
||||||||||||||||||
|
|
Name |
|
|
|
|
|
|
|
Dosage |
|
|
|
Route |
|
|
Frequency |
|
|
|
|
|
|
Type |
|
|
|
Frequency |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
16. |
Treatment Plan (Attach copy of order sheet if more convenient or other pertinent documents) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||
|
Previous Hospitalizations:____________________________ Rehabilitative Services:__________________________ Other Health Services:_________________________ |
||||||||||||||||||||||||||||||||||||||||
|
Hospital Diagnosis: 1)_________________________________ 2) Secondary______________________________ 3) Other_____________________________________ |
||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
17. Anticipated Dates of Hospitalization: |
__________/________ |
|
|
|
18. |
Level of Care Recommended: |
Hospital |
Nursing Facility |
|
|
IC/MR Facility |
|||||||||||||||||||||||||||||
|
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
19. |
Type of Recommendation: |
|
|
|
20. Patient Transferred from (check one): |
|
21. Length of Time Care Needed _____Months |
|
22. Is patient free of |
||||||||||||||||||||||||||||||||
|
|
Initial |
|
|
|
|
|
|
|
Hospital |
|
Another NF |
|
|
|
1) |
Permanent |
|
|
|
|
|
|
|
communicable diseases? |
||||||||||||||||
|
|
Change Level of Care |
|
|
|
Private Pay |
|
Lives at home |
|
|
|
2) |
Temporary _______ estimated |
|
|
Yes |
|
No |
|||||||||||||||||||||||
|
|
Continued Placement |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
23. |
This patient’s condition |
could |
could not be managed by |
|
|
24. Physician’s Name (Print): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
provision of |
Community Care or |
|
Home Health Services |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician’s Address (Print): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
25. |
I certify that this patient requires the level of care provided |
|
|
26. Date signed by Physician |
|
27. |
|
Physician’s Licensure No. |
|
28. Physician’s Telephone #: |
|||||||||||||||||||||||||||||||
|
by a nursing facility, IC/MR facility, or hospital |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|||||||||||||
|
______________________________________Physician’s Signature |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
Section C– Evaluation of Nursing Care Needed (check appropriate box only) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
29. |
Nutrition |
|
|
|
30. |
|
|
Bowel |
|
|
|
|
|
|
31. Cardiopulmonary Status |
|
32. |
|
|
Mobility |
|
33. |
|
|
|
Behavioral Status |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
Regular |
|
|
|
|
Age Dependent |
|
|
|
|
Monitoring |
|
|
|
|
|
|
Prosthesis |
|
|
|
|
Agitated |
|
|
|
||||||||||||||
|
|
Diabetic Shots |
|
|
|
|
Incontinence |
|
|
|
|
|
|
|
|
|
|
|
|
Splints |
|
|
|
|
Cooperative |
|
|
||||||||||||||
|
|
|
|
|
Incontinent - Age > 3 years |
|
CP Monitor |
|
|
|
|
|
|
Unable to ambulate > |
|
Alert |
|
|
|
||||||||||||||||||||||
|
|
Tube feeding |
|
|
|
|
Colostomy |
|
|
|
|
|
|
Pulse Ox |
|
|
|
|
|
|
18 months old |
|
|
|
|
Developmental Delay |
|||||||||||||||
|
|
|
|
|
Continent |
|
|
|
|
|
|
Vital signs > 2/days |
|
|
|
|
Wheel chair |
|
|
|
|
Mental Retardation |
|||||||||||||||||||
|
|
Slow Feeder |
|
|
|
|
Other ________________ |
|
Therapy |
|
|
|
|
|
|
Normal |
|
|
|
|
Behavioral Problems |
||||||||||||||||||||
|
|
FTT or Premature |
|
|
|
|
|
|
|
|
|
|
|
|
|
Oxygen |
|
|
|
|
|
|
|
|
|
|
|
|
|
(please describe, if checked) |
|||||||||||
|
|
Hyperal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Home Vent |
|
|
|
|
|
|
|
|
|
|
|
|
|
Suicidal |
|
|
|
|||||||
|
|
IV Use |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Trach |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hostile |
|
|
|
|||||
|
|
Medications/GT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Nebulizer Tx |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
Meds |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Suctioning |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Chest - Physical Tx |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Room Air |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
34. |
Integument System |
|
|
35. |
|
|
Urogenital |
|
|
|
|
36. |
|
|
Surgery |
|
|
|
37. |
|
Therapy/Visits |
|
38. |
|
Neurological Status |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
Burn Care |
|
|
|
|
Dialysis in home |
|
|
|
|
Level 1 (5 or > surgeries) |
|
Day care Services |
|
|
|
|
Deaf |
|
|
|
||||||||||||||||||||
|
Sterile Dressings |
|
|
|
|
Ostomy |
|
|
|
|
|
|
Level II (< 5 surgeries) |
|
|
|
|
High Tech - 4 or more |
|
Blind |
|
|
|
||||||||||||||||||
|
Decubiti |
|
|
|
|
Incontinent – Age > 3 years |
|
None |
|
|
|
|
|
|
|
|
times per week |
|
|
|
|
Seizures |
|
|
|
||||||||||||||||
|
Bedridden |
|
|
|
|
Catheterization |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Low Tech – 3 or less times |
|
Neurological Deficits |
|||||||||||||||||
|
|
|
|
|
Continent |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
per week or MD visits > 4 |
|
Paralysis |
|
|
|
||||||||||||||
|
|
Normal |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
per month |
|
|
|
|
Normal |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
None |
|
|
|
|
|
|
|
|
|
|
|
|||
39. |
Other Therapy Visits |
|
|
|
|
|
|
|
|
|
|
|
|
|
40. |
|
|
Remarks |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
Five days per week |
|
Less than 5 days per week |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
41. |
|
|
|
|
|
|
|
|
42. |
|
|
Date Signed |
43. Print Name of MD or RN:_____________________________ |
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature of MD or RN:_______________________________ |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DO NOT WRITE BELOW THIS LINE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
44. |
Continued Stay Review Date: |
|
|
|
|
|
|
|
Admission Date ___________________ Approved for ______________Days or ___________Months |
||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
45. |
Are nursing services, rehabilitative services or other health related services |
|
|
|
46A. State Authority MH & MR Screening) |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
requested ordinarily provided in an institution? |
Yes |
No |
|
|
|
Level I/II |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Restricted Auth. Code |
|
|
Date |
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
46B. This is not a |
|
|
|
|
|
|
|
|||||||||||
47. |
Hospitalization Precertification |
|
|
Met |
|
Not |
Met |
|
|
|
|
|
|
|
|
|
Restricted Auth. Code |
|
|
Date |
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
48. |
Level of Care Recommended by Contractor |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
Hospital |
Nursing Facility |
IC/MR Facility |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
49. |
Approval Period |
|
|
|
|
|
|
|
|
50. Signature (Contractor) |
|
51. Date |
|
|
|
|
|
|
52. Attachments (Contractor) |
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
________________ |
|
/ |
/ |
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||