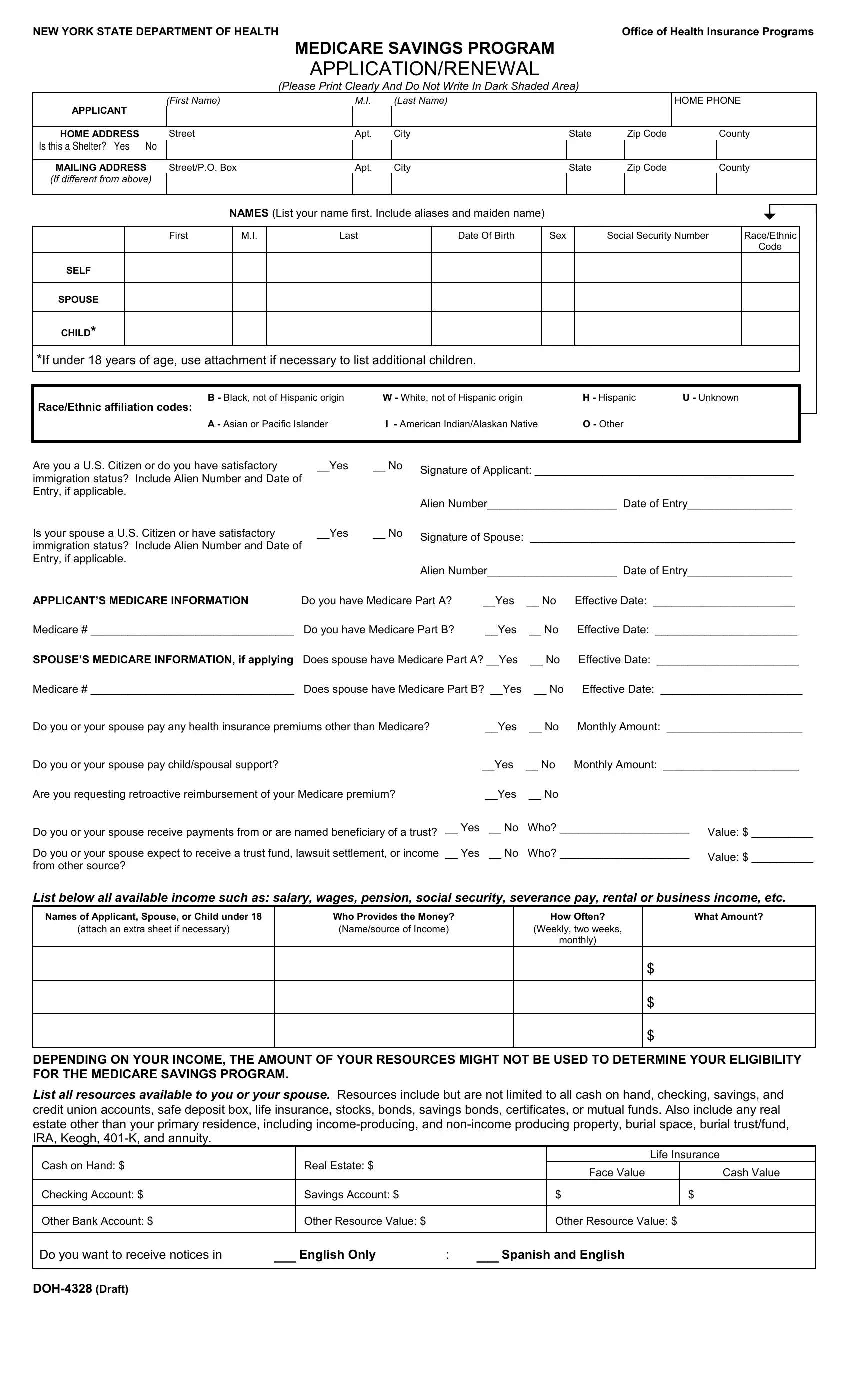
The Medicare Savings Program (MSP) serves as a crucial financial support system for eligible individuals striving to cover their Medicare expenses. Managed by the New York State Department of Health, the MSP application and renewal process is facilitated through the completion of the DOH 4328 form. This comprehensive document is designed to collect essential information from applicants, including personal details, home and mailing addresses, racial and ethnic backgrounds, citizenship or immigration status, and detailed Medicare information for both the applicant and, if applicable, their spouse. Additionally, the form inquires about other health insurance premiums, child or spousal support payments, and any anticipated reimbursements for Medicare premiums already paid. A noteworthy aspect of the DOH 4328 form is its emphasis on the applicant's financial resources and income, which can include salary, pension, social security, and income from property or businesses, to name a few. Furthermore, it stresses the importance of reporting any changes in circumstances that could affect eligibility for the program. The form also contains a certification section where applicants must affirm the accuracy of the information provided, acknowledge the potential for investigation, and consent to the use of their data for eligibility determination purposes. With a focus on fairness, the application process adheres to a non-discrimination policy, ensuring that applicants are evaluated without regard to race, color, sex, disability, or other protected characteristics. The DOH 4328 form epitomizes a structured approach to assisting individuals in navigating the complexities of healthcare financing, underscoring the government's commitment to accessibility and equity within its healthcare system.
| Question | Answer |
|---|---|
| Form Name | Form Doh 4328 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Keogh, doh 4328 pdf, New_York, SSN |
NEW YORK STATE DEPARTMENT OF HEALTH |
Office of Health Insurance Programs |
|
MEDICARE SAVINGS PROGRAM |
|
APPLICATION/RENEWAL |
(Please Print Clearly And Do Not Write In Dark Shaded Area)
|
(First Name) |
M.I. |
(Last Name) |
|
|
HOME PHONE |
|
APPLICANT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HOME ADDRESS |
Street |
Apt. |
City |
State |
Zip Code |
|
County |
IS THIS A SHELTER? YES NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MAILING ADDRESS |
Street/P.O. Box |
Apt. |
City |
State |
Zip Code |
|
County |
(If different from above) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAMES (List your name first. Include aliases and maiden name) |
|
|
6 |
||
|
|
|
|
|||
|
|
|
|
|
|
|
First |
M.I. |
Last |
Date Of Birth |
Sex |
Social Security Number |
Race/Ethnic |
|
|
|
|
|
|
Code |
SELF |
|
|
|
|
|
|
SPOUSE
CHILD*
*If under 18 years of age, use attachment if necessary to list additional children.
B - Black, not of Hispanic origin |
W - White, not of Hispanic origin |
|
H - Hispanic |
U - Unknown |
|
|||||
Race/Ethnic affiliation codes: |
|
|
|
|
|
|
|
|
|
|
A - Asian or Pacific Islander |
I - American Indian/Alaskan Native |
O - Other |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
Are you a U.S. Citizen or do you have satisfactory |
__Yes |
__ No |
Signature of Applicant: __________________________________________ |
|||||||
immigration status? Include Alien Number and Date of |
|
|||||||||
|
|
|
|
|
|
|
|
|
||
Entry, if applicable. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Alien Number_____________________ Date of Entry_________________ |
|||||||
Is your spouse a U.S. Citizen or have satisfactory |
__Yes |
__ No |
Signature of Spouse: ___________________________________________ |
|||||||
immigration status? Include Alien Number and Date of |
|
|||||||||
|
|
|
|
|
|
|
|
|
||
Entry, if applicable. |
|
|
|
|
|
|
|
|
|
|
|
|
|
Alien Number_____________________ Date of Entry_________________ |
|||||||
APPLICANT’S MEDICARE INFORMATION |
Do you have Medicare Part A? |
__Yes |
__ No |
Effective Date: _______________________ |
||||||
Medicare # _________________________________ |
Do you have Medicare Part B? |
__Yes |
__ No |
Effective Date: _______________________ |
||||||
SPOUSE’S MEDICARE INFORMATION, if applying |
Does spouse have Medicare Part A? __Yes |
__ No |
Effective Date: _______________________ |
|||||||
Medicare # _________________________________ |
Does spouse have Medicare Part B? __Yes |
__ No |
Effective Date: _______________________ |
|||||||
Do you or your spouse pay any health insurance premiums other than Medicare? |
|
__Yes |
__ No |
Monthly Amount: ______________________ |
||||||
Do you or your spouse pay child/spousal support? |
|
|
|
|
__Yes |
__ No |
Monthly Amount: ______________________ |
|||
Are you requesting retroactive reimbursement of your Medicare premium? |
|
|
__Yes |
__ No |
|
|
|
|
||
Do you or your spouse receive payments from or are named beneficiary of a trust? |
__ Yes |
__ No |
Who? _____________________ Value: $ __________ |
|||||||
Do you or your spouse expect to receive a trust fund, lawsuit settlement, or income |
__ Yes |
__ No |
Who? _____________________ |
Value: $ __________ |
||||||
from other source? |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
List below all available income such as: salary, wages, pension, social security, severance pay, rental or business income, etc.
Names of Applicant, Spouse, or Child under 18 |
Who Provides the Money? |
How Often? |
What Amount? |
(attach an extra sheet if necessary) |
(Name/source of Income) |
(Weekly, two weeks, |
|
|
|
monthly) |
|
|
|
|
$ |
|
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
$ |
|
|
|
|
DEPENDING ON YOUR INCOME, THE AMOUNT OF YOUR RESOURCES MIGHT NOT BE USED TO DETERMINE YOUR ELIGIBILITY FOR THE MEDICARE SAVINGS PROGRAM.
List all resources available to you or your spouse. Resources include but are not limited to all cash on hand, checking, savings, and credit union accounts, safe deposit box, life insurance, stocks, bonds, savings bonds, certificates, or mutual funds. Also include any real estate other than your primary residence, including
|
|
|
|
|
|
Life Insurance |
|
Cash on Hand: $ |
|
Real Estate: $ |
|
|
Face Value |
|
Cash Value |
|
|
|
|
|
|
||
Checking Account: $ |
|
Savings Account: $ |
|
|
$ |
|
$ |
|
|
|
|
|
|
|
|
Other Bank Account: $ |
|
Other Resource Value: $ |
|
|
Other Resource Value: $ |
||
|
|
|
|
|
|
|
|
Do you want to receive notices in |
__ English Only |
: |
__ Spanish and English |
|
|
||
|
|
|
|
|
|
|
|

PAYMENT OF YOUR MEDICARE PREMIUM IS A MEDICAID BENEFIT
PENALTIES: I understand that my application may be investigated, and I agree to cooperate in such an investigation. Federal and State laws provide for penalties of fine, imprisonment or both if you do not tell the truth when you apply for Medicaid benefits or at any time when you are questioned about your eligibility, or cause someone else not to tell the truth regarding your application or your continuing eligibility. Penalties also apply if you conceal or fail to disclose facts regarding your initial and continuing eligibility for Medicaid or if you conceal or fail to disclose facts that would effect the right of someone for whom you have applied to obtain or continue to receive Medicaid benefits; and such benefits must be used by the other person and not for yourself.
CHANGES: I agree to inform the agency promptly of any change in my needs, income, property, living arrangements or address to the best of my knowledge or belief.
SOCIAL SECURITY NUMBER (SSN): If you are applying for the Medicare Savings Program, you must
report your SSN, unless you are a pregnant woman. The laws requiring this are: 18NYCRR Sections
351.2and
CERTIFICATION OF CITIZENSHIP & IMMIGRATION STATUS: I certify, under the penalty of perjury, by signing my name on this application, that I, and/or any person for whom I am signing is a U.S. citizen or national of the United States or has satisfactory immigration status. I understand that information about me will be submitted to the United States Citizenship and Immigration Services (USCIS) for verification of my immigration status, if applicable. I further understand that the use or disclosure of information about me is restricted to persons and organizations directly connected with the verification of immigration status and the administration and enforcement of the provisions of the Medicaid program.
CERTIFICATION: In signing this application, I swear and affirm that the information I have given or will give to the Department of Social Services as a basis for Medicaid is correct. I also assign to the Department of Social Services any rights I have to pursue support from persons having legal responsibility for my support and to pursue other
CONSENT: I understand that by signing this application/certification form I agree to any investigation made by the Department of Social Services to verify or confirm the information I have given or any other investigation made by them in connection with my request for Medicaid. If additional information is requested, I will provide it.
Applicant/Representative
Signature X ______________________________________________________ Date _____________
Spouse Signature X _______________________________________________ Date _____________
Representative Address, Phone Number and Relationship ___________________________________________________
_____________________________________________________________________________________________________
If after reading and completing this form, you decide that you DO NOT want to apply for the Medicare Savings Program please sign on the following line.
I consent to withdraw my application ___________________________________ Date ____________
SIGNATURE OF PERSON WHO OBTAINED ELIGIBILITY INFORMATION: |
DATE: |
EMPLOYED BY: |
|
|
|
|
|||||
x |
|
|
|
|
|
|
|
|
|
|
|
Eligibility Determined By Worker: |
________________________ |
Eligibility Approved By: |
________________________ |
||||||||
|
|
|
|
(DATE) |
|
|
|
|
(DATE) |
||
CENTRAL/OFFICE |
APPLICATION DATE |
|
UNIT ID |
|
WORKER ID |
CASE TYPE |
CASE NO |
|
|
|
REUSE IND. |
|
|
|
|
|
|
|
|
|
|
|
|
CASE NAME |
|
|
DISTRICT |
|
|
REGISTRY NO. |
|
VER. |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REASON CODE |
PROXY: |
|
|
||
Effective Date ___________ MA Disp. |
Denial |
|
Withdrawal |
|
|
Yes |
|
No |
|||
|
|
|
|
|
|
|
|
|
|
|
|