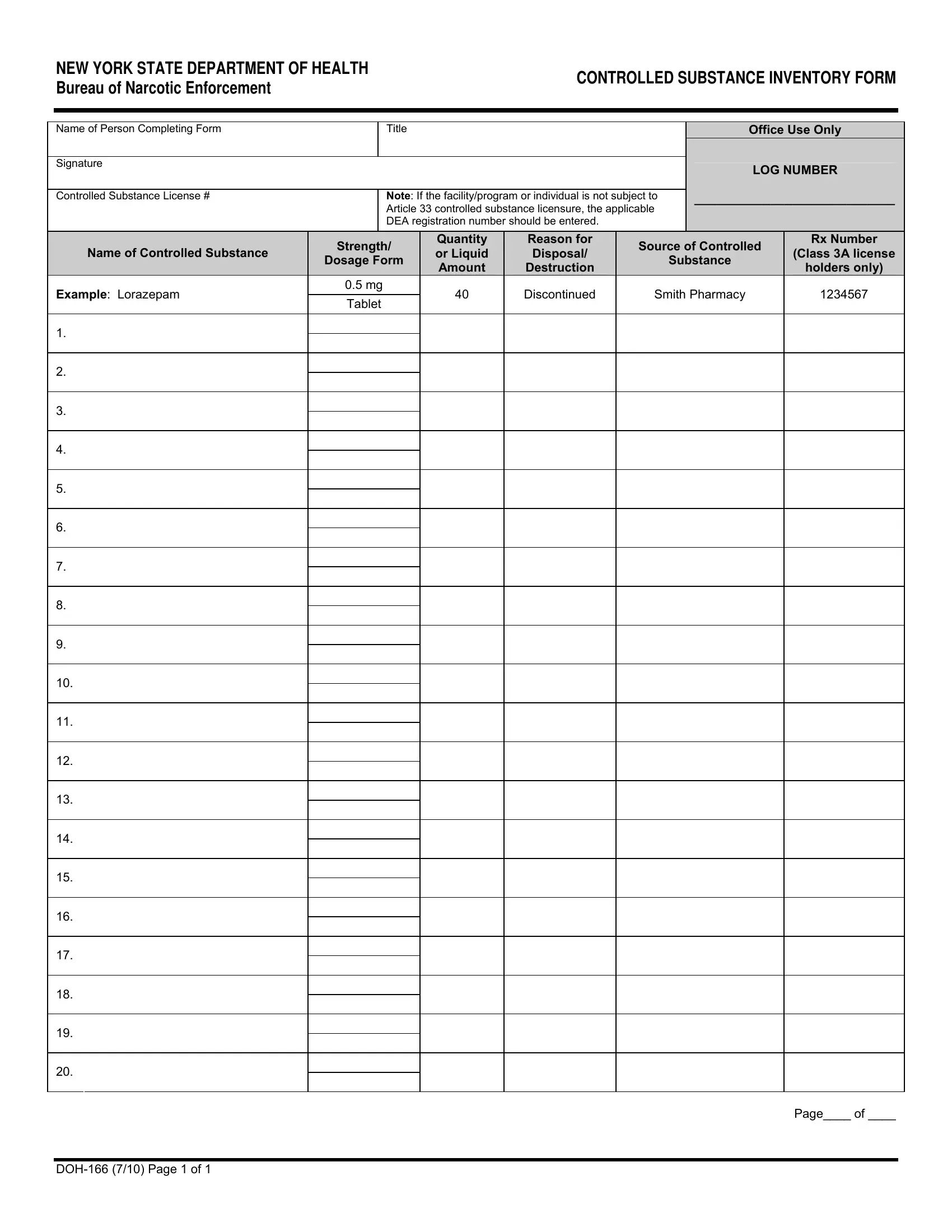
In the realm of healthcare and pharmaceuticals, maintaining precise records of controlled substances is not only best practice but also a legal requirement. The Doh 166 form, issued by the New York State Department of Health Bureau of Narcotic Enforcement, plays a crucial role in this process. This form, known as the Controlled Substance Inventory Form, demands meticulous attention to detail from the individuals completing it. Its primary purpose is to catalogue controlled substances, tracking their strength, quantity, and the reason for their disposal or destruction. Additionally, it necessitates the inclusion of the controlled substance license number or, in cases where Article 33 licensing is not applicable, the Drug Enforcement Administration (DEA) registration number. This comprehensive approach ensures that every controlled substance within a facility or held by an individual practitioner is accounted for, aiming to prevent misuse and enhance safety. The Doh 166 form exemplifies the intersection of regulatory compliance and public health, reinforcing the stringent measures in place to monitor the flow of potent medications within the healthcare system.
| Question | Answer |
|---|---|
| Form Name | Doh 166 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | new york state doh 166, controlled substance inventory form, controlled substance tracking form, doh 166http web4 hillside com applications |
