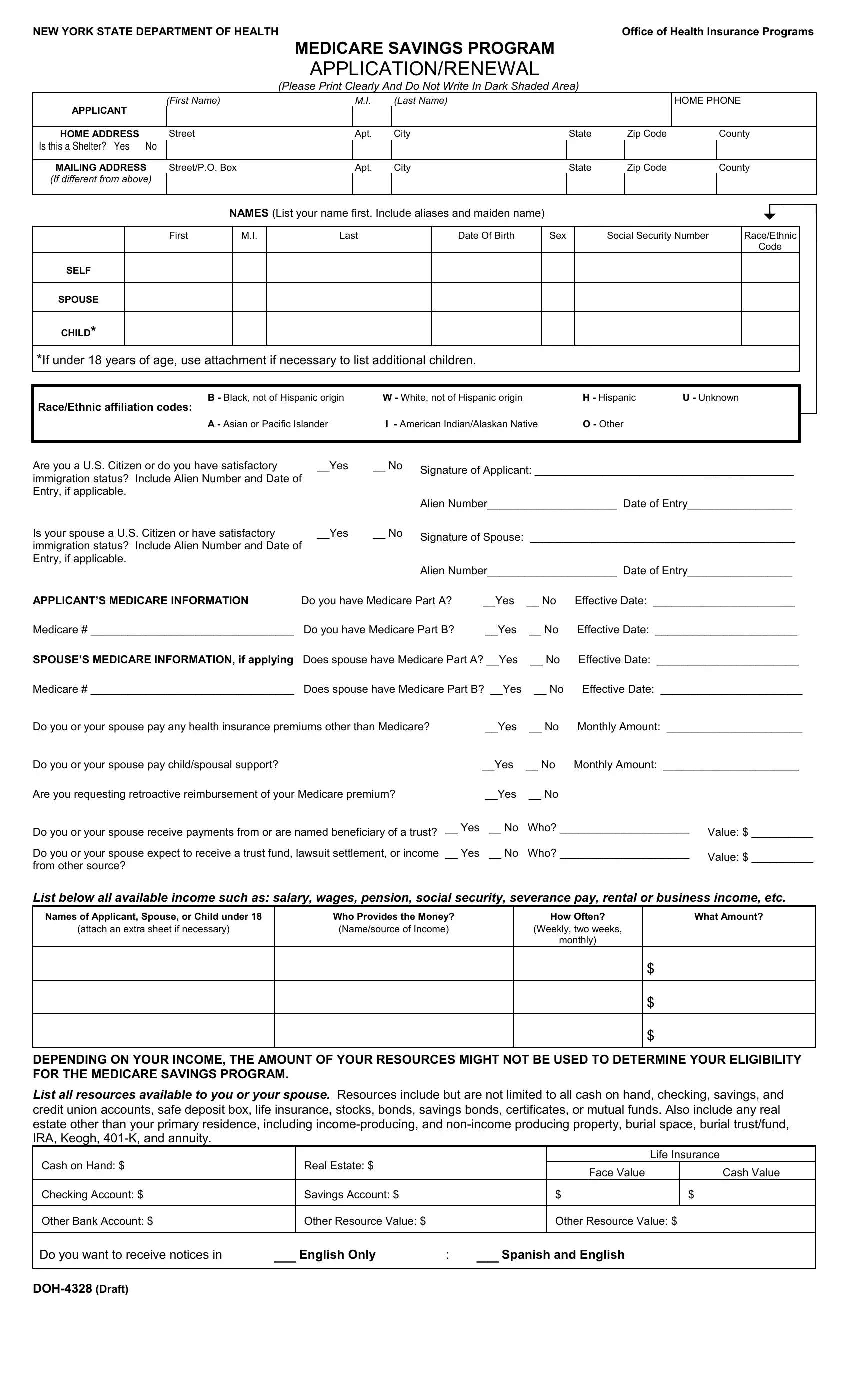
The Medicare Savings Program (MSP) serves as a crucial financial support system for eligible individuals striving to cover their Medicare expenses. Managed by the New York State Department of Health, the MSP application and renewal process is facilitated through the completion of the DOH 4328 form. This comprehensive document is designed to collect essential information from applicants, including personal details, home and mailing addresses, racial and ethnic backgrounds, citizenship or immigration status, and detailed Medicare information for both the applicant and, if applicable, their spouse. Additionally, the form inquires about other health insurance premiums, child or spousal support payments, and any anticipated reimbursements for Medicare premiums already paid. A noteworthy aspect of the DOH 4328 form is its emphasis on the applicant's financial resources and income, which can include salary, pension, social security, and income from property or businesses, to name a few. Furthermore, it stresses the importance of reporting any changes in circumstances that could affect eligibility for the program. The form also contains a certification section where applicants must affirm the accuracy of the information provided, acknowledge the potential for investigation, and consent to the use of their data for eligibility determination purposes. With a focus on fairness, the application process adheres to a non-discrimination policy, ensuring that applicants are evaluated without regard to race, color, sex, disability, or other protected characteristics. The DOH 4328 form epitomizes a structured approach to assisting individuals in navigating the complexities of healthcare financing, underscoring the government's commitment to accessibility and equity within its healthcare system.
| Question | Answer |
|---|---|
| Form Name | Form Doh 4328 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Keogh, doh 4328 pdf, New_York, SSN |
