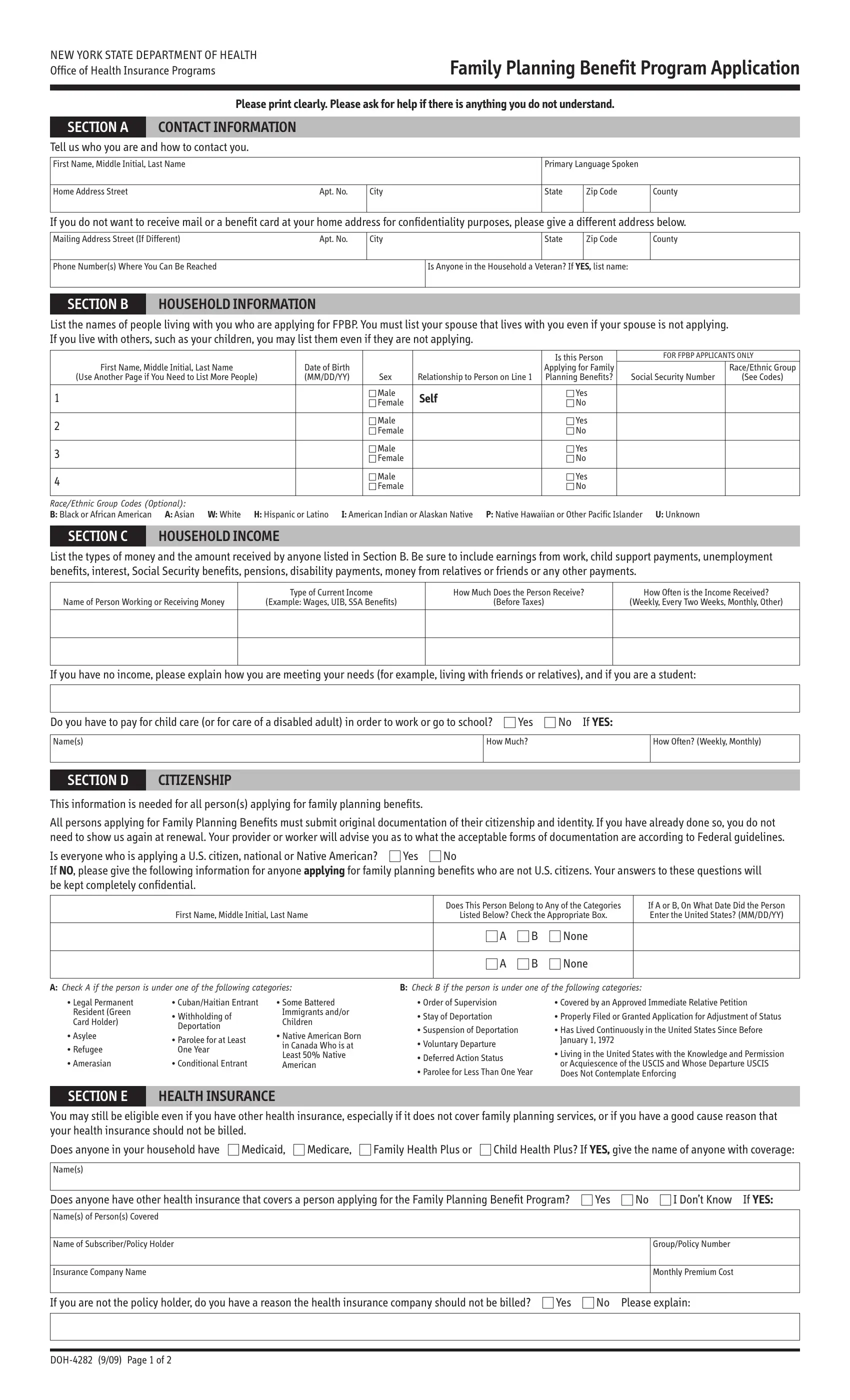
Navigating the complexities of healthcare and family planning services can be a daunting task, particularly for residents of New York State seeking assistance through public health programs. The DOH-4282 form, a critical document within the New York State Department of Health's Office of Health Insurance Programs, serves as a key to accessing the Family Planning Benefit Program (FPBP). Designed to be user-friendly, the form requires applicants to provide detailed contact information, household information, including the composition and income levels, citizenship details, and information regarding any existing health insurance coverages. This comprehensive approach is aimed at identifying eligibility for the FPBP, which provides a range of family planning services to individuals. Applicants are guided through a series of sections that meticulously collect data necessary for the evaluation of their application, including an emphasis on confidentiality and the importance of accurate information. Meanwhile, terms, rights, and responsibilities articulated at the conclusion of the application underscore the legal and ethical underpinning of the process, emphasizing non-discrimination, the necessity of truthful declarations, and the critical role of social security numbers in verifying eligibility and facilitating health benefits. This form illustrates the State's efforts to streamline access to health services, while also safeguarding the integrity and efficiency of its health care system.
| Question | Answer |
|---|---|
| Form Name | Form Doh 4282 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 1396a, SSA, New_York, UIB |
