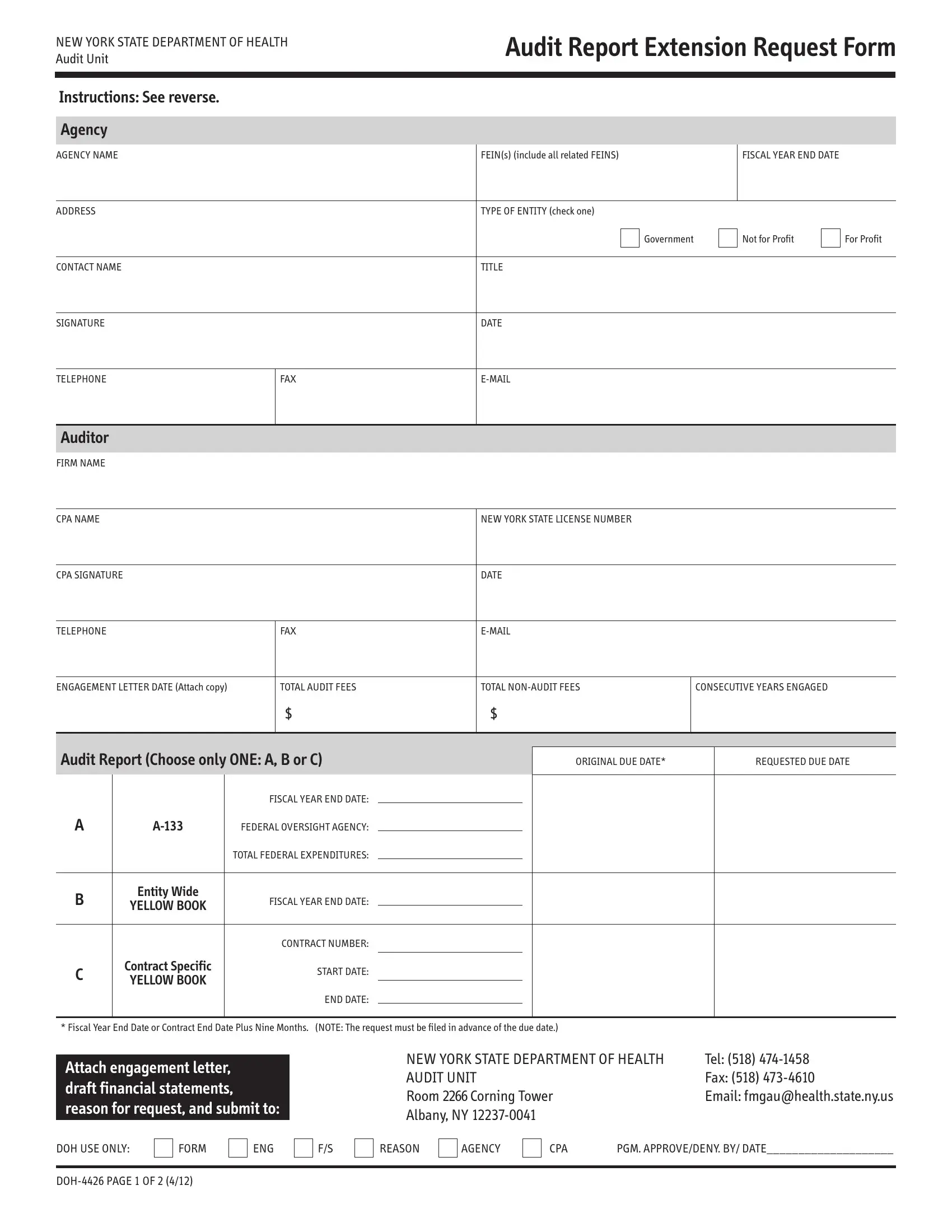
Managing compliance and ensuring financial accountability are critical aspects that agencies operating in New York State must navigate diligently. The New York State Department of Health's Audit Report Extension Request Form, known as DOH-4426, serves as a vital tool in this process, offering agencies a structured pathway to request additional time for submitting their audit reports. This form caters to various types of entities, including government, not-for-profit, and for-profit organizations, and requires comprehensive information such as agency name, fiscal year-end date, and contact details. Moreover, it necessitates details about the audit firm engaged, including the CPA’s name and New York State license number, along with the engagement letter date, total audit fees, and the number of years the auditor has been engaged. The form also distinguishes between different reports, such as A-133, entity-wide, or contract-specific audits, asking for original and requested due dates. Additionally, the instructions emphasize the importance of attaching an auditor’s engagement letter, a separate letter stating the reason for the extension request, and, for A-133 reports, specific documentation related to federal funding. Submission details, including where and how to submit the request, underscore the procedural nature of acquiring an audit report extension, reflecting the Department's commitment to oversight and financial integrity within the state.
| Question | Answer |
|---|---|
| Form Name | Form Doh 4426 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | doh 4426 nys department of health audit unit form |
NEW YORK STATE DEPARTMENT OF HEALTH Audit Unit
Audit Report Extension Request Form
Instructions: See reverse.
Agency
AGENCY NAME
FEIN(s) (include all related FEINS)
FISCAL YEAR END DATE
ADDRESS
TYPE OF ENTITY (check one)
Government
Not for Profit
For Profit
CONTACT NAME
TITLE
SIGNATURE
DATE
TELEPHONE
FAX
Auditor
FIRM NAME
CPA NAME |
|
|
|
|
NEW YORK STATE LICENSE NUMBER |
|
||
|
|
|
|
|
|
|
|
|
CPA SIGNATURE |
|
|
|
|
DATE |
|
||
|
|
|
|
|
|
|
|
|
TELEPHONE |
|
|
FAX |
|
||||
|
|
|
|
|
|
|
|
|
ENGAGEMENT LETTER DATE (Attach copy) |
|
TOTAL AUDIT FEES |
TOTAL |
CONSECUTIVE YEARS ENGAGED |
||||
|
|
|
$ |
|
$ |
|
|
|
|
|
|
|
|
|
|
||
Audit Report (Choose only ONE: A, B or C) |
|
|
|
|
||||
|
|
ORIGINAL DUE DATE* |
REQUESTED DUE DATE |
|||||
|
|
|
|
|
|
|
|
|
A |
FISCAL YEAR END DATE: |
|
|
|
|
|
||
|
|
|
|
|
||||
FEDERAL OVERSIGHT AGENCY: |
|
|
|
|
|
|||
|
|
TOTAL FEDERAL EXPENDITURES: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B |
Entity Wide |
FISCAL YEAR END DATE: |
|
|
|
|
|
|
YELLOW BOOK |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CONTRACT NUMBER: |
|
|
|
|
|
|
Contract Specific |
|
|
|
|
|
|
|
C |
|
START DATE: |
|
|
|
|
||
YELLOW BOOK |
|
|
|
|
|
|||
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
END DATE:
* Fiscal Year End Date or Contract End Date Plus Nine Months. (NOTE: The request must be filed in advance of the due date.)
Attach engagement letter, draft financial statements, reason for request, and submit to:
NEW YORK STATE DEPARTMENT OF HEALTH |
Tel: (518) |
AUDIT UNIT |
Fax: (518) |
Room 2266Corning Tower |
Email: fmgau@health.state.ny.us |
Albany, NY |
|
DOH USE ONLY:
FORM
ENG
F/S
REASON
AGENCY
CPA |
PGM. APPROVE/DENY. BY/ DATE____________________ |
Instructions
1.Attach a copy of the Auditor’s Engagement Letter. The letter must reference the report type, scope and intended completion date.
2.Attach a separate letter describing the good cause reason for the request. The letter must specifically explain why the report will not be completed by the due date. If the agency is unprepared, the letter must include a list of tasks yet to be completed. If the auditor is unavail- able, the request must include a copy of the unaudited financial statements. The letter must be typed on agency letterhead, addressed to the Department, include a commitment to meet the revised date, and include the signature of the agency official responsible for preparing the financial statements.
3.For
a.Attach a copy of the draft Schedule of Expenditures of Federal Awards.
b.If all Federal funding is from a
c.Submit the Form, including the Engagement Letter and the reason for the request, to your Federal cognizant agency. Your cognizant agency is the Federal agency which provides your agency the most Federal funding, direct or
USDA
Regional Audit Director, USDA FNS 10 Causeway St, Rm 501 Boston MA 02222
Tel (617)
DHHS
Manager, DHHS Audit Resolution
1100 Walnut Street, Room 850
Kansas City MO 64106
Tel (816)
Email – jfisher@oig.hhs.gov
HUD
National Single Audit Coordinator, HUD
Wanamaker Building, Suite 1005, 100 Penn Square East
Philadelphia, PA
Tel (215)
If your agency is not listed, refer to: http:/www.whitehouse.gov/omb/circulars/a133_Compliance/08/appx_3/pdf
ii.Submit a copy to NYSDOH at the address below.
iii.If the Federal agency approves the request, submit a copy of the Federal approval letter to NYSDOH at the address below.
4.For Yellow Book
NEW YORK STATE DEPARTMENT OF HEALTH |
Tel: (518) |
AUDIT UNIT |
Fax: (518) |
Room 2266Corning Tower |
Email: fmgau@health.state.ny.us |
Albany, NY |
|