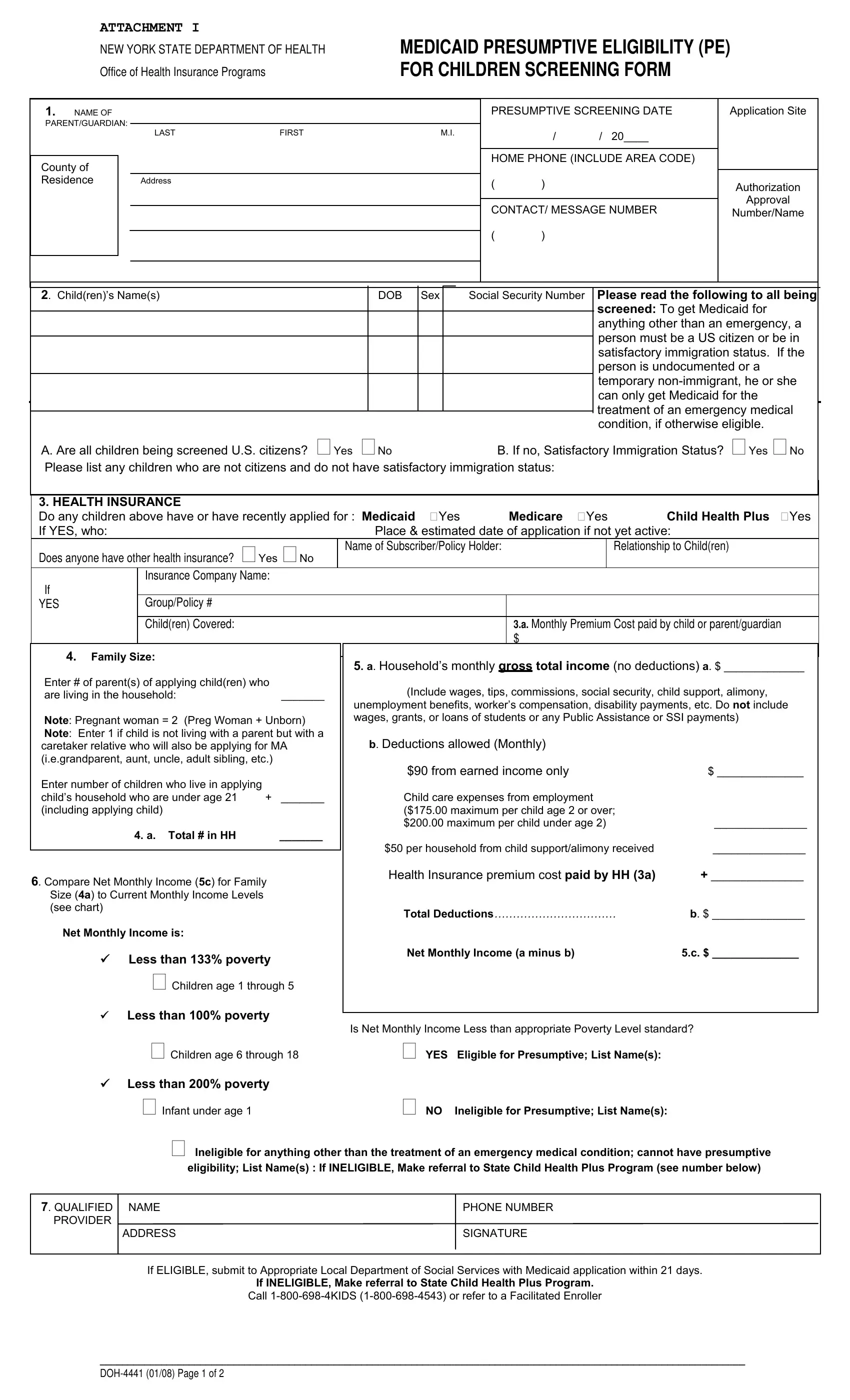
Ensuring that children receive the medical attention they need is a priority that necessitates an understanding of the complexities surrounding Medicaid Presumptive Eligibility (PE) as elucidated in the DOH 4441 form, issued by the New York State Department of Health. This form acts as a critical bridge for children under the Medicaid Presumptive Eligibility program, guiding screening agencies through the process of determining temporary eligibility for Medicaid based on preliminary information. It requires detailed inputs regarding the child's guardian, their residency, citizenship, and existing health coverage, alongside family size and household income to ascertain if the children meet the eligibility criteria. Notably, it underscores the necessity for caregivers to provide accurate information about the child's citizenship or satisfactory immigration status, highlighting a nuanced approach to healthcare provision that considers immigration status while prioritizing emergency medical care for all. This document is instrumental not only in streamlining the initial steps towards securing Medicaid but also in laying down a procedural framework that ensures rapid access to healthcare services for children, thereby reflecting a commitment to uphold children's health rights without immediate, exhaustive document verification. As such, the DOH 4441 form embodies a significant aspect of public health policy, recognizing the urgency of healthcare needs among children and facilitating a responsive mechanism to address these needs through Medicaid's Presumptive Eligibility pathway.
| Question | Answer |
|---|---|
| Form Name | Form Doh 4441 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Enroller, NYSDOH, presumptive eligibility medicaid filler pdf online printabe, LDSS |
ATTACHMENT I
NEW YORK STATE DEPARTMENT OF HEALTH
Office of Health Insurance Programs
MEDICAID PRESUMPTIVE ELIGIBILITY (PE) FOR CHILDREN SCREENING FORM
1. NAME OF |
|
|
|
|
|
|
|
|
|
|
|
PRESUMPTIVE SCREENING DATE |
|
Application Site |
||||||||
PARENT/GUARDIAN: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
LAST |
|
FIRST |
|
|
|
M.I. |
|
|
|
/ |
/ |
|
20____ |
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HOME PHONE (INCLUDE AREA CODE) |
|
|||||||
County of |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Residence |
|
|
|
Address |
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
Authorization |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Approval |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CONTACT/ MESSAGE NUMBER |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Number/Name |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. Child(ren)’s Name(s) |
|
|
|
|
DOB |
Sex |
|
Social Security Number |
|
Please read the following to all being |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
screened: To get Medicaid for |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
anything other than an emergency, a |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
person must be a US citizen or be in |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
satisfactory immigration status. If the |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
person is undocumented or a |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
temporary |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
can only get Medicaid for the |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
treatment of an emergency medical |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
condition, if otherwise eligible. |
||||
A. Are all children being screened U.S. citizens? Yes No |
|
|
|
|
|
B. If no, Satisfactory Immigration Status? Yes No |
||||||||||||||||
Please list any children who are not citizens and do not have satisfactory immigration status: |
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3. HEALTH INSURANCE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Do any children above have or have recently applied for : Medicaid |
Yes |
|
Medicare Yes |
Child Health Plus Yes |
||||||||||||||||||
If YES, who: |
|
|
|
|
|
|
Place & estimated date of application if not yet active: |
|
|
|||||||||||||
Does anyone have other health insurance? Yes No |
|
Name of Subscriber/Policy Holder: |
|
|
|
Relationship to Child(ren) |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
Insurance Company Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
YES |
|
Group/Policy # |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
Child(ren) Covered: |
|
|
|
|
|
|
|
|
|
|
|
3.A. Monthly Premium Cost paid by child or parent/guardian |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ __________________________ |
|
|
||||
4. Family Size: |
|
|
|
5. a. Household’s monthly gross total income (no deductions) a. $ _____________ |
||||||||||||||||||
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|||||||||||||||
Enter # of parent(s) of applying child(ren) who |
|
|
|
(Include wages, tips, commissions, social security, child support, alimony, |
||||||||||||||||||
are living in the household: |
|
_______ |
|
|
||||||||||||||||||
|
|
unemployment benefits, worker’s compensation, disability payments, etc. Do not include |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|||||||||||||||
Note: Pregnant woman = 2 (Preg Woman + Unborn) |
|
wages, grants, or loans of students or any Public Assistance or SSI payments) |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Note: Enter 1 if child is not living with a parent but with a |
|
|
b. Deductions allowed (Monthly) |
|
|
|
|
|
|
|||||||||||||
caretaker relative who will also be applying for MA |
|
|
|
|
|
|
|
|
||||||||||||||
(i.e.grandparent, aunt, uncle, adult sibling, etc.) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
$90 from earned income only |
|
|
|
|
$ ______________ |
||||||||
Enter number of children who live in applying |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
child’s household who are under age 21 |
+ |
_______ |
|
|
Child care expenses from employment |
|
|
|
|
|
|
|||||||||||
(including applying child) |
|
|
|
|
($175.00 maximum per child age 2 or over; |
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
$200.00 maximum per child under age 2) |
|
_______________ |
|||||||||||
|
|
|
4. a. Total # in HH |
|
_______ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$50 per household from child support/alimony received |
_______________ |
||||||||||||
|
|
|
|
|
|
|
|
|
||||||||||||||
6. Compare Net Monthly Income (5c) for Family |
|
|
|
Health Insurance premium cost paid by HH (3a) |
+ _______________ |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Size (4a) to Current Monthly Income Levels |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
(see chart) |
|
|
|
|
|
|
Total Deductions…………………………… |
b. $ _______________ |
||||||||||||||
|
|
|
|
|
|
|
|
|
||||||||||||||
Net Monthly Income is: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
9 Less than 133% poverty |
|
|
|
Net Monthly Income (a minus b) |
|
|
|
|
5.c. $ ______________ |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
Children age 1 through 5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
9 Less than 100% poverty |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
Is Net Monthly Income Less than appropriate Poverty Level standard? |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
Children age 6 through 18 |
|
|
YES |
Eligible for Presumptive; List Name(s): |
|
|
||||||||||||
9Less than 200% poverty
Infant under age 1 |
NO Ineligible for Presumptive; List Name(s): |
Ineligible for anything other than the treatment of an emergency medical condition; cannot have presumptive eligibility; List Name(s) : If INELIGIBLE, Make referral to State Child Health Plus Program (see number below)
7. QUALIFIED NAME |
PHONE NUMBER |
PROVIDER |
|
ADDRESS |
SIGNATURE |
If ELIGIBLE, submit to Appropriate Local Department of Social Services with Medicaid application within 21 days.
If INELIGIBLE, Make referral to State Child Health Plus Program.
Call
____________________________________________________________________________________________________________________
NEW YORK STATE DEPARTMENT OF HEALTH
Office of Health Insurance Programs
MEDICAID PRESUMPTIVE ELIGIBILITY (PE) FOR CHILDREN SCREENING FORM
Instructions for Completing PE for Children Screening Form
Section 1:
Name: List name of parent(s)/guardian(s) of the applying child(ren)
Address: List the address where the child(ren) live(s) including house number, street name, apt number, city, and zip code
County of Residence: Enter county in which above address is located
Presumptive Screening Date: List today’s date
Home Phone / Contact/Message Number: Enter home, contact/message number
Application Site: List the name of the Qualified Entity Site
Authorization Number/Name: Call NYSDOH to obtain authorization number for children who screen eligible. Document the name of the person who provided you with the number.
Section 2:
Child(ren)’s Names: List all children who are being screened for PE for Children
Enter SSN (if known), SSN or proof of application for SSN will have to be provided for full Medicaid determination
A/B: Citizenship/Immigration Status: Check boxes as appropriate. Explain that Medicaid is available to people who are US Citizens or have satisfactory immigration status. Others may receive treatment only for an emergency medical condition. If unsure of the child(ren)’s status, ask if they have any of the following: a Green Card, a Passport, a Visa or any other document that allows them to stay here indefinitely. Also ask if they are working with immigration services to get permanent status.
Section 3:
Health Insurance: Complete as much information as known. Inquire about recent applications for Child Health Plus, Medicaid, and Family Health Plus. If yes, indicate when and where the application was taken.
Section 4:
Family Size: Enter numbers to identify number of persons living in the household. If the mother of the applying child is pregnant, count as 2 (mom plus the unborn child). Count the legal spouse and/or father of the child, if they live in the household. Count 1 for Caretaker Relative (if no parents live in the household) and if they will also be applying for Medicaid. Count all of the children under age 21 in the household whether or not they are applying. Do not count persons who receive Temporary Cash Assistance or SSI cash assistance. Total number of household members will be recorded on line 4.a.
Section 5:
Income: On line 5a. enter the total amount of the monthly gross (before taxes and deductions) household income. Verification is not required for PE. Weekly wages are converted to monthly by multiplying by 4.3333. Do not count grants, loans, student’s wages, Temporary Cash Assistance or SSI Cash Assistance. Enter caretaker relative’s income if they are in the household count and are applying for MA. Enter monthly amounts as allowed in b. Child care expenses may be deducted only if parent/guardian is employed. Only one $50 deduction per household is allowed if anyone (or more than one person) in the HH receives child support payments. Enter the total monthly premium paid out for health insurance premiums. Add deductions and enter on line 5.b. The Net Monthly Income amount, entered on line 5.c., is the figure that results when the total allowable deductions (line 5b) is subtracted from the household gross income (line 5a).
Section 6:
Compare the net monthly income with the income standards chart for the appropriate household size (4.a.) and percentage of the Federal Poverty Level for the age of each child. If the child(ren) is found to be eligible, the corresponding box(es) is checked, the child(ren)’s name(s) is listed and a Presumptive Eligibility Screening Determination letter is given to the applying parent or guardian with the names of the children who are Presumptively Eligible for Medicaid. This letter advises households of next steps to take to apply for ongoing Medicaid. This completed screening form, an accompanying Medicaid application, determination letter and all documentation are forwarded to the appropriate county Local Department of Social Services (LDSS) within 21 days for further review and a determination for ongoing Medicaid.
If any child applying is ineligible, list the name of the child(ren) that is ineligible and refer to the phone numbers at the bottom of the screening sheet for information on applying for Child Health Plus, and/or refer to the nearest Facilitated Enroller for application assistance. If all children on the screening are ineligible, do not send the PE screening form to the LDSS, but retain copies in a locked, secure area.
Section 7:
Qualified Provider must enter their name, address, telephone number, and sign the bottom of the form.
____________________________________________________________________________________________________________________