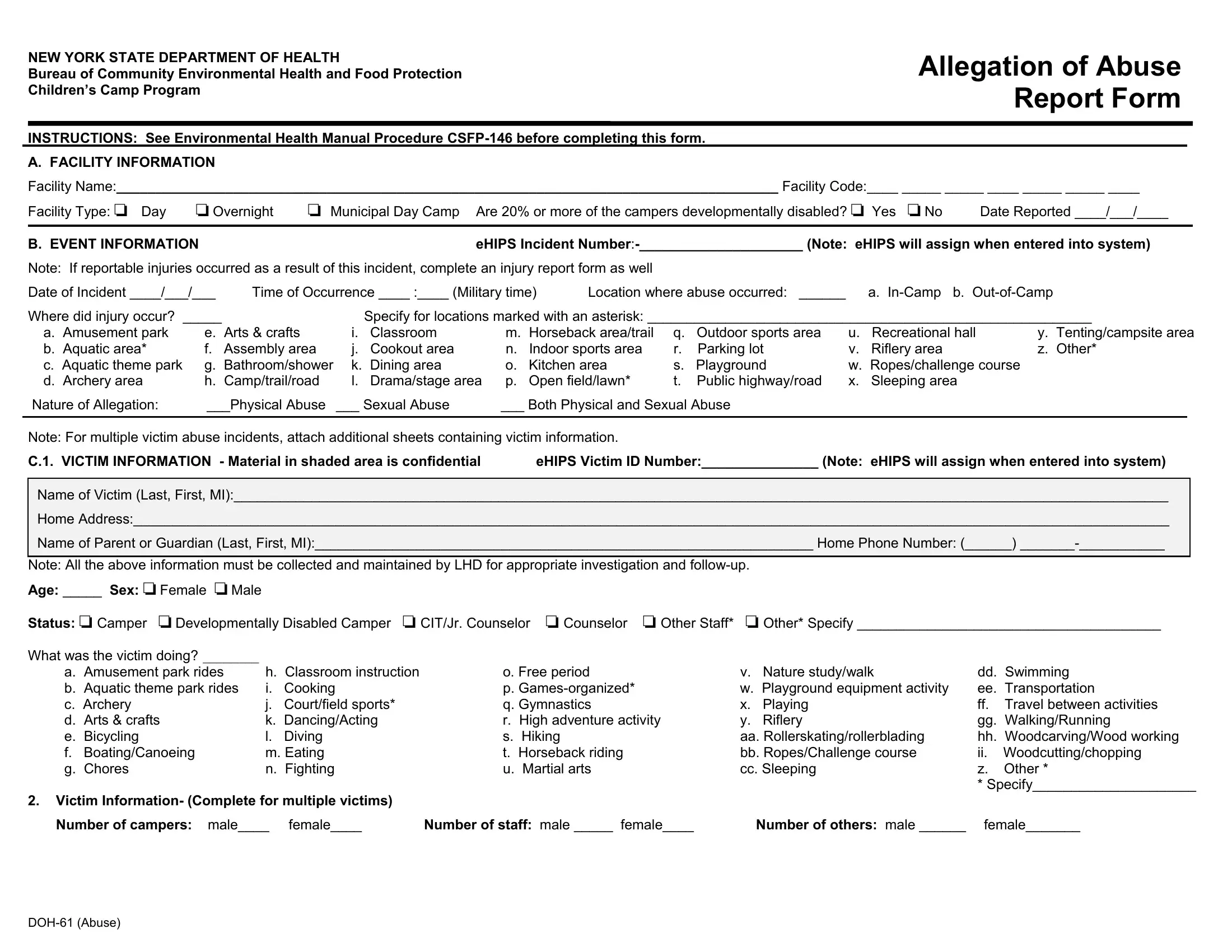
The New York State Department of Health has taken significant steps to ensure the safety and well-being of children attending various camps through the implementation of the DOH-61 form, also known as the Children’s Camp Program Report Form. This crucial document serves as a comprehensive method for reporting and addressing allegations of abuse within children's camp settings. The form meticulously gathers detailed information about the facility, including specifics about whether it operates during the day or overnight and if it caters to developmentally disabled campers. It further delves into the particulars of the event, requiring information on when and where the abuse occurred, and demands a narrative of the incident to better understand the circumstances surrounding the allegation. Victim details are treated with utmost confidentiality, ensuring the sensitive handling of their identities and the specifics of their experiences. Additionally, the form prompts for an evaluation of the supervision provided during the incident, scrutinizing whether the activity was adequately addressed in the camp's written plan, and assessing the qualifications and actions of the staff present. Alleged perpetrator information is captured with care to facilitate a thorough investigation. The completion of this form triggers a process that may involve an on-site investigation by the Local Health Department, ensuring that each allegation is followed up with appropriate action. The narrative section demands a succinct yet detailed description of the incident, conclusions drawn, and recommendations for the camp to implement, aiming to prevent such incidents in the future and ensure compliance with Subpart 7-2 regulations. This structured approach underscores the Department's commitment to the safety of children in these environments, pushing for accountability and continuous improvement in camp safety standards.
| Question | Answer |
|---|---|
| Form Name | Form Doh 61 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | camp alleg of abuse rptform environmental health manual procedure csfp 146 form |
NEW YORK STATE DEPARTMENT OF HEALTH |
Allegation of Abuse |
Bureau of Community Environmental Health and Food Protection |
|
Children’s Camp Program |
Report Form |
|
|
INSTRUCTIONS: See Environmental Health Manual Procedure |
|
A. FACILITY INFORMATION |
|
Facility Name:_____________________________________________________________________________________ Facility Code:____ _____ _____ ____ _____ _____ ____
|
Facility Type: |
Day |
Overnight |
Municipal Day Camp |
Are 20% or more of the campers developmentally disabled? |
|
Yes |
No |
Date Reported ____/___/____ |
||||||||
|
|
|
|
|
|
|
|
|
|||||||||
|
B. EVENT INFORMATION |
|
|
|
|
eHIPS Incident |
|||||||||||
|
Note: If reportable injuries occurred as a result of this incident, complete an injury report form as well |
|
|
|
|
|
|
|
|
||||||||
|
Date of Incident ____/___/___ |
Time of Occurrence ____ :____ (Military time) |
Location where abuse occurred: ______ |
|
a. |
||||||||||||
|
Where did injury occur? _____ |
|
|
Specify for locations marked with an asterisk: _________________________________________________________ |
|||||||||||||
|
a. Amusement park |
e. Arts & crafts |
i. |
Classroom |
m. Horseback area/trail |
q. |
Outdoor sports area |
u. |
Recreational hall |
y. Tenting/campsite area |
|||||||
|
b. Aquatic area* |
f. |
Assembly area |
j. |
Cookout area |
n. |
Indoor sports area |
r. |
Parking lot |
v. |
Riflery area |
z. Other* |
|||||
|
c. Aquatic theme park |
g. Bathroom/shower k. |
Dining area |
o. |
Kitchen area |
s. |
Playground |
w. |
Ropes/challenge course |
||||||||
|
d. Archery area |
h. Camp/trail/road |
l. |
Drama/stage area p. |
Open field/lawn* |
t. |
Public highway/road |
x. |
Sleeping area |
|
|
|
|||||
|
Nature of Allegation: |
___Physical Abuse |
___ Sexual Abuse |
___ Both Physical and Sexual Abuse |
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Note: For multiple victim abuse incidents, attach additional sheets containing victim information.
C.1. VICTIM INFORMATION - Material in shaded area is confidential eHIPS Victim ID Number:_______________ (Note: eHIPS will assign when entered into system)
Name of Victim (Last, First, MI):________________________________________________________________________________________________________________________
Home Address:_____________________________________________________________________________________________________________________________________
Name of Parent or Guardian (Last, First, MI):________________________________________________________________ Home Phone Number: (______)
Note: All the above information must be collected and maintained by LHD for appropriate investigation and
Age: _____ Sex: |
Female |
Male |
|
|
|
|
|
|
|
|
|
Status: |
Camper |
Developmentally Disabled Camper |
CIT/Jr. Counselor |
Counselor |
Other Staff* |
Other* Specify _______________________________________ |
|||||
What was the victim doing? ________ |
|
|
|
|
|
|
|
|
|||
a. Amusement park rides |
|
h. Classroom instruction |
o. Free period |
v. |
Nature study/walk |
dd. Swimming |
|||||
b. Aquatic theme park rides |
i. |
Cooking |
p. |
w. |
Playground equipment activity |
ee. Transportation |
|||||
c. Archery |
|
|
j. |
Court/field sports* |
q. Gymnastics |
x. |
Playing |
ff. |
Travel between activities |
||
d. Arts & crafts |
|
k. |
Dancing/Acting |
r. High adventure activity |
y. |
Riflery |
gg. |
Walking/Running |
|||
e. Bicycling |
|
|
l. |
Diving |
s. Hiking |
|
aa. Rollerskating/rollerblading |
hh. |
Woodcarving/Wood working |
||
f. |
Boating/Canoeing |
|
m. Eating |
t. Horseback riding |
bb. Ropes/Challenge course |
ii. |
Woodcutting/chopping |
||||
g. |
Chores |
|
|
n. Fighting |
u. Martial arts |
cc. Sleeping |
z. |
Other * |
|||
* Specify_____________________
2.Victim Information- (Complete for multiple victims)
Number of campers: male____ female____ |
Number of staff: male _____ female____ |
Number of others: male ______ female_______ |
D. |
SUPERVISION |
|
|
|
|
1. |
Supervision during incident (indicate as many as apply) _____ _____ _____ _____ |
|
|
|
|
|
a. Activity inadequately addressed in |
d. No staff present |
h. Staff orientation/training for activity not |
k. Written plan not followed |
|
|
the written plan |
e. Quality of supervision adequate |
|
documented/received |
|
|
b. Activity not addressed in the written plan |
f. Quality of supervision inadequate |
i. |
Supervision ratio inadequate |
z. Other * |
|
c. Camper orientation for activity not |
g. Staff not trained/knowledgeable as |
j. |
Supervision ratio correct |
* Specify____________________________ |
|
documented/received |
per the written plan |
|
|
___________________________________ |
E. |
ALLEGED PERPETRATOR INFORMATION: |
Attach additional sheets if multiple perpetrators. |
|
||
Name: _______________________________________
Age:________
Sex ________
Information in shaded area is confidential
Status: |
CIT/Jr. Counselor |
Counselor |
No relation to camp |
Trespasser |
Visitor |
|
|
|
|||||
|
Camper |
Dev. Disabled Camper |
Other Staff* |
|
Unknown |
*Specify_________________________ |
F. INVESTIGATION |
|
|
|
|
|
|
Was an |
Yes |
No |
Date of |
|||
Did the Local Health Department conduct a telephone |
Yes |
No |
Date of |
|||
G.NARRATIVE- Do not include the full names of people involved with the incident. Use the first and last name initials or other similar code.
Allegation of Abuse- Provide a description of the event, conclusions and DOH recommendations: Include statements pertaining to Subpart
the acceptability/implementation of the camp written plan. Recommendations should include whether or not administrative action against the camp will be taken as well as the steps that must be taken to prevent similar incidents in the future. See Environmental Health Procedure
_______________________________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________________________________
Information received by: _________________________________ |
Title:____________________________________ |
Report reviewed by: ____________________________________ |
Title:____________________________________ |