
Should you wish to fill out ok disability placard application form, there's no need to download and install any software - just try our online tool. Our team is continuously working to improve the tool and make it even better for clients with its cutting-edge functions. Take full advantage of today's modern opportunities, and discover a trove of new experiences! If you're seeking to start, this is what you will need to do:
Step 1: Firstly, access the pdf editor by clicking the "Get Form Button" in the top section of this webpage.
Step 2: When you launch the editor, you will notice the form prepared to be filled out. In addition to filling in different blank fields, you may also do various other things with the file, namely putting on your own text, editing the initial text, adding images, affixing your signature to the PDF, and a lot more.
This form will need you to enter some specific details; to ensure correctness, you need to consider the following steps:
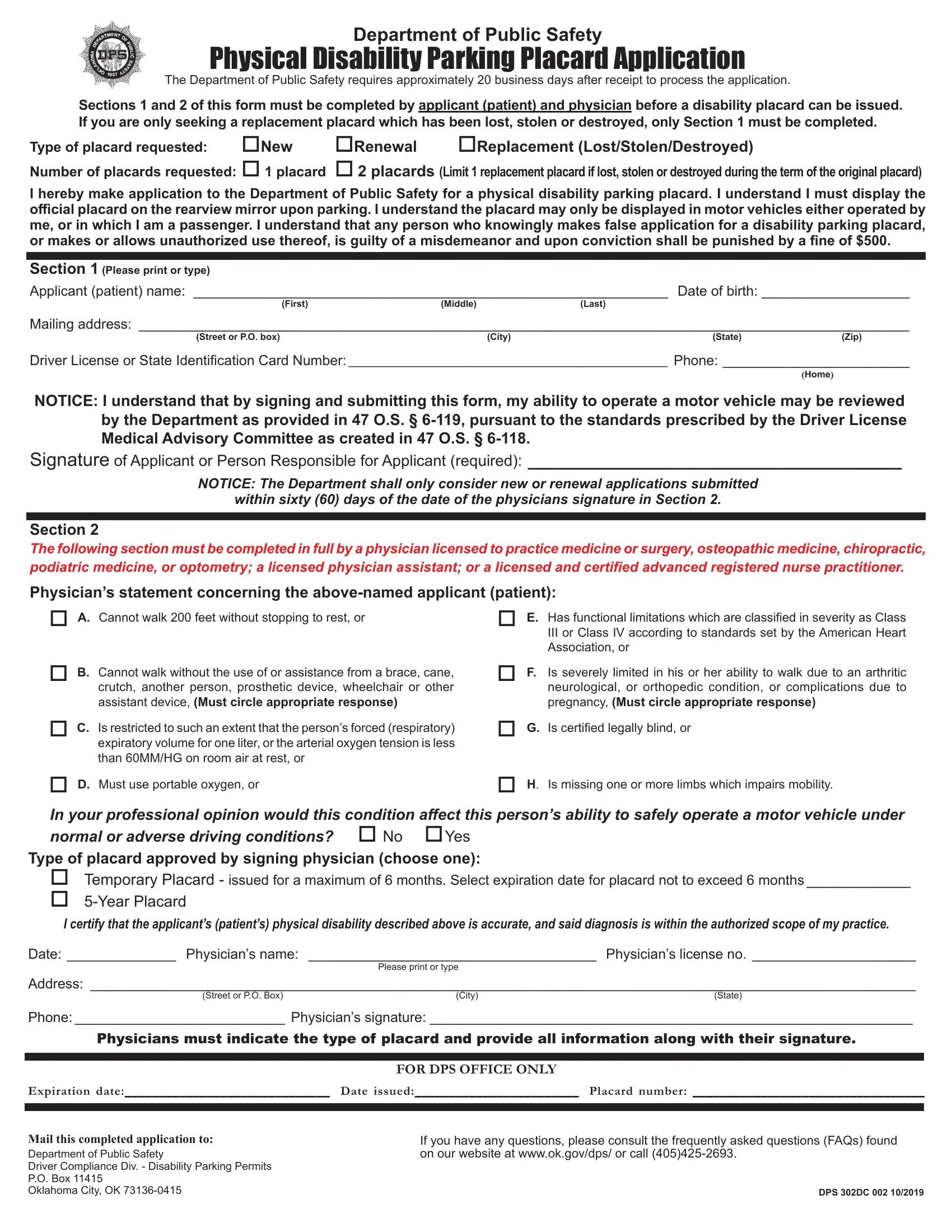
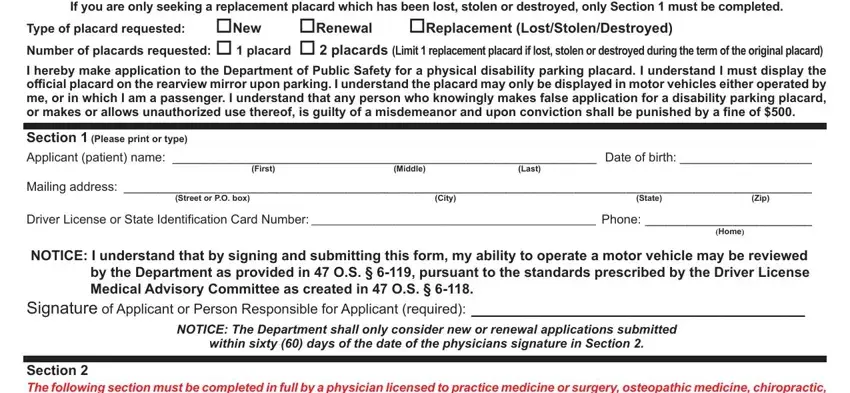
1. When submitting the ok disability placard application form, be sure to include all needed blanks within its relevant part. It will help to speed up the work, which allows your details to be handled efficiently and appropriately.
2. Once the previous part is finished, you need to add the essential particulars in Section The following section, A Cannot walk feet without, E Has functional limitations, B Cannot walk without the use of, crutch another person prosthetic, Is severely limited in his or her, C Is restricted to such an extent, G Is certified legally blind or, D Must use portable oxygen or, In your professional opinion, H Is missing one or more limbs, No Yes Type of placard approved, Temporary Placard issued for a, I certify that the applicants, and Date Physicians name Physicians so that you can move on further.
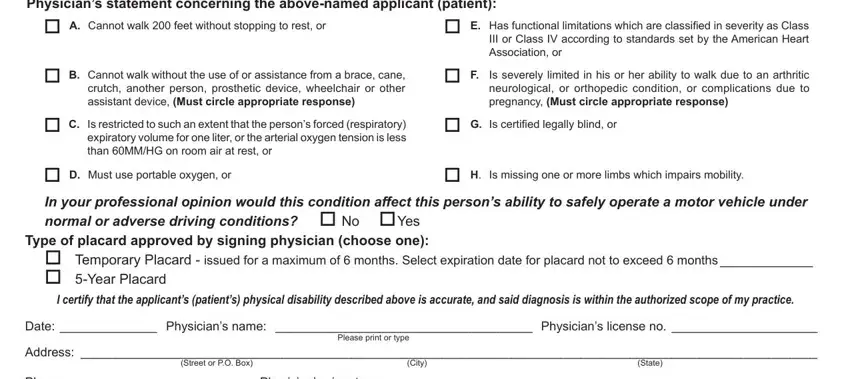
Be really attentive when filling out Section The following section and B Cannot walk without the use of, since this is the part in which many people make errors.
Step 3: Look through the details you've inserted in the blank fields and click on the "Done" button. Sign up with FormsPal today and immediately access ok disability placard application form, set for download. Every last change made is conveniently preserved , so that you can customize the form later as needed. FormsPal ensures your data privacy by using a secure method that never saves or shares any sort of private information used in the PDF. You can relax knowing your documents are kept safe each time you work with our services!