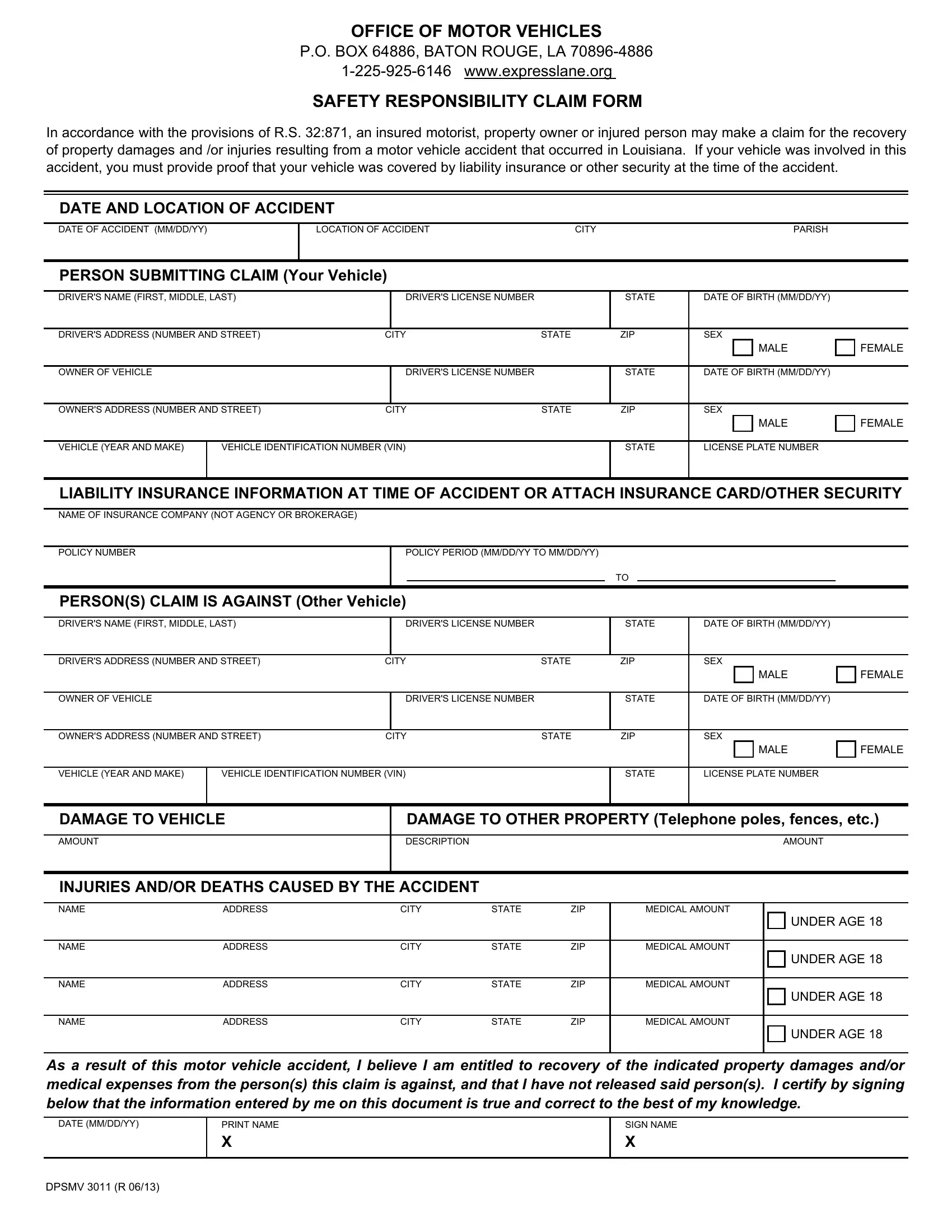
The Dpsmv 3011 form serves as a critical tool for individuals in Louisiana seeking to navigate the aftermath of a motor vehicle accident. This document is designed to facilitate the process of claiming recovery for property damages and/or injuries that occur as a result of such incidents. Managed by the Office of Motor Vehicles and in accordance with R.S. 32:871, it provides a structured means for insured motorists, property owners, or injured parties to formally submit their claims. The form requires detailed information regarding the accident, including the date, location, and parties involved, both the claimant and the alleged responsible party. It also asks for specifics about the vehicle(s) involved, insurance coverage at the time of the accident, the extent of vehicle and property damage, and a thorough account of injuries or deaths that resulted. This form underscores the importance of proving liability insurance or other security was in effect at the time of the accident to proceed with a claim. By completing and submitting this form, individuals assert their belief in their entitlement to recover damages or medical expenses due to the incident, a process underscored by the requirement to certify the truthfulness of the information provided. This guide intends to demystify the process, offering clarity and support to those navigating the potentially complex waters of post-accident claims in Louisiana.
| Question | Answer |
|---|---|
| Form Name | Form Dpsmv 3011 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | SUBMITTING, Louisiana, resulting, expresslane |