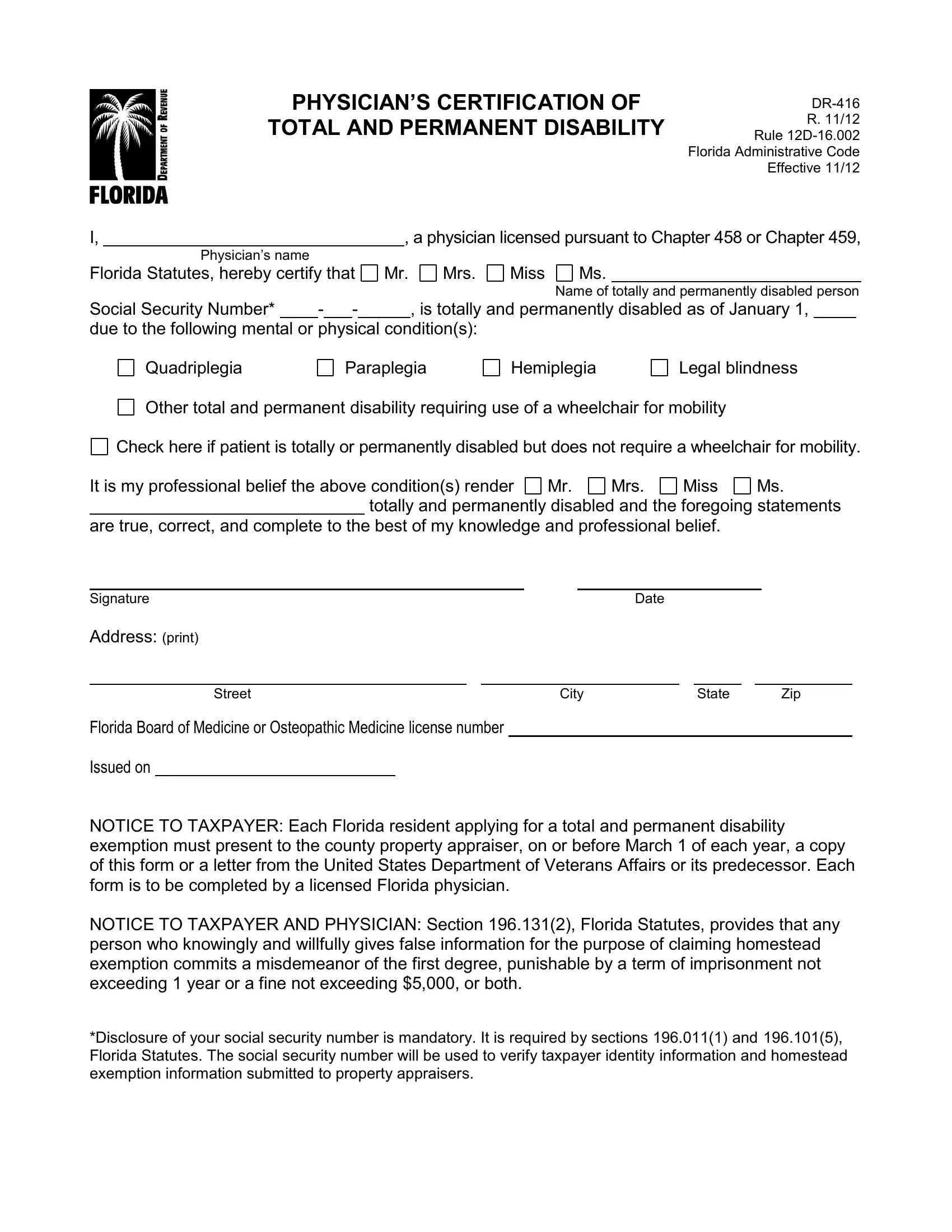
The Dr 416 form, a crucial document within the state of Florida, serves as a formal certification by licensed physicians, under the auspices of Chapters 458 or 459 of the Florida Statutes, affirming a patient's status as being totally and permanently disabled. This form specifically addresses individuals suffering from a range of conditions including quadriplegia, paraplegia, hemiplegia, legal blindness, or other disabilities that necessitate the use of a wheelchair for mobility, although it also accommodates those whose disabilities do not require such aids. The form plays a pivotal role in the application process for a total and permanent disability exemption, which must be presented to the county property appraiser by March 1st of each year to potentially qualify for tax exemptions. Accuracy and honesty in completing this form are paramount, as falsely claiming a homestead exemption is considered a misdemeanor of the first degree, a crime punishable by significant fines or imprisonment. The form also underscores the importance of social security numbers for verifying the identity of the taxpayer and the legitimacy of the exemption claim, illustrating the balance between privacy concerns and the necessity of transparency in claims related to tax exemptions.
| Question | Answer |
|---|---|
| Form Name | Form Dr 416 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | fl dr 416 form, florida dr 416 form, dr 416 disability form, florida total permanent |
PHYSICIAN’S CERTIFICATION OF
TOTAL AND PERMANENT DISABILITY
R. 11/12
Rule
Florida Administrative Code
Effective 11/12
I, |
|
|
|
|
|
, a physician licensed pursuant to Chapter 458 or Chapter 459, |
||||||||
|
Physician’s name |
|
|
|
|
|
|
|
|
|
|
|
|
|
Florida Statutes, hereby certify that |
Mr. |
Mrs. |
Miss |
Ms. |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
Name of |
totally and permanently disabled person |
||
Social Security Number* |
|
- |
|
- |
|
|
, is totally and permanently disabled as of January 1, |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||
due to the following mental or |
physical condition(s): |
|
|
|
|
|
||||||||
Quadriplegia
Paraplegia
Hemiplegia
Legal blindness
Other total and permanent disability requiring use of a wheelchair for mobility
Check here if patient is totally or permanently disabled but does not require a wheelchair for mobility.
It is my professional belief the above condition(s) render |
Mr. |
Mrs. |
Miss |
|
Ms. |
||||||
|
totally and permanently disabled and the foregoing statements |
||||||||||
are true, correct, and complete to the |
best of my knowledge and professional belief. |
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
Signature |
|
|
Date |
|
|
|
|
|
|||
Address: (print) |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|||
Street |
|
|
City |
|
|
State |
|
|
Zip |
||
Florida Board of Florida Board of Medicine or Osteopathic Medicine license number
Issued on
NOTICE TO TAXPAYER: Each Florida resident applying for a total and permanent disability exemption must present to the county property appraiser, on or before March 1 of each year, a copy of this form or a letter from the United States Department of Veterans Affairs or its predecessor. Each form is to be completed by a licensed Florida physician.
NOTICE TO TAXPAYER AND PHYSICIAN: Section 196.131(2), Florida Statutes, provides that any person who knowingly and willfully gives false information for the purpose of claiming homestead exemption commits a misdemeanor of the first degree, punishable by a term of imprisonment not exceeding 1 year or a fine not exceeding $5,000, or both.
*Disclosure of your social security number is mandatory. It is required by sections 196.011(1) and 196.101(5), Florida Statutes. The social security number will be used to verify taxpayer identity information and homestead exemption information submitted to property appraisers.