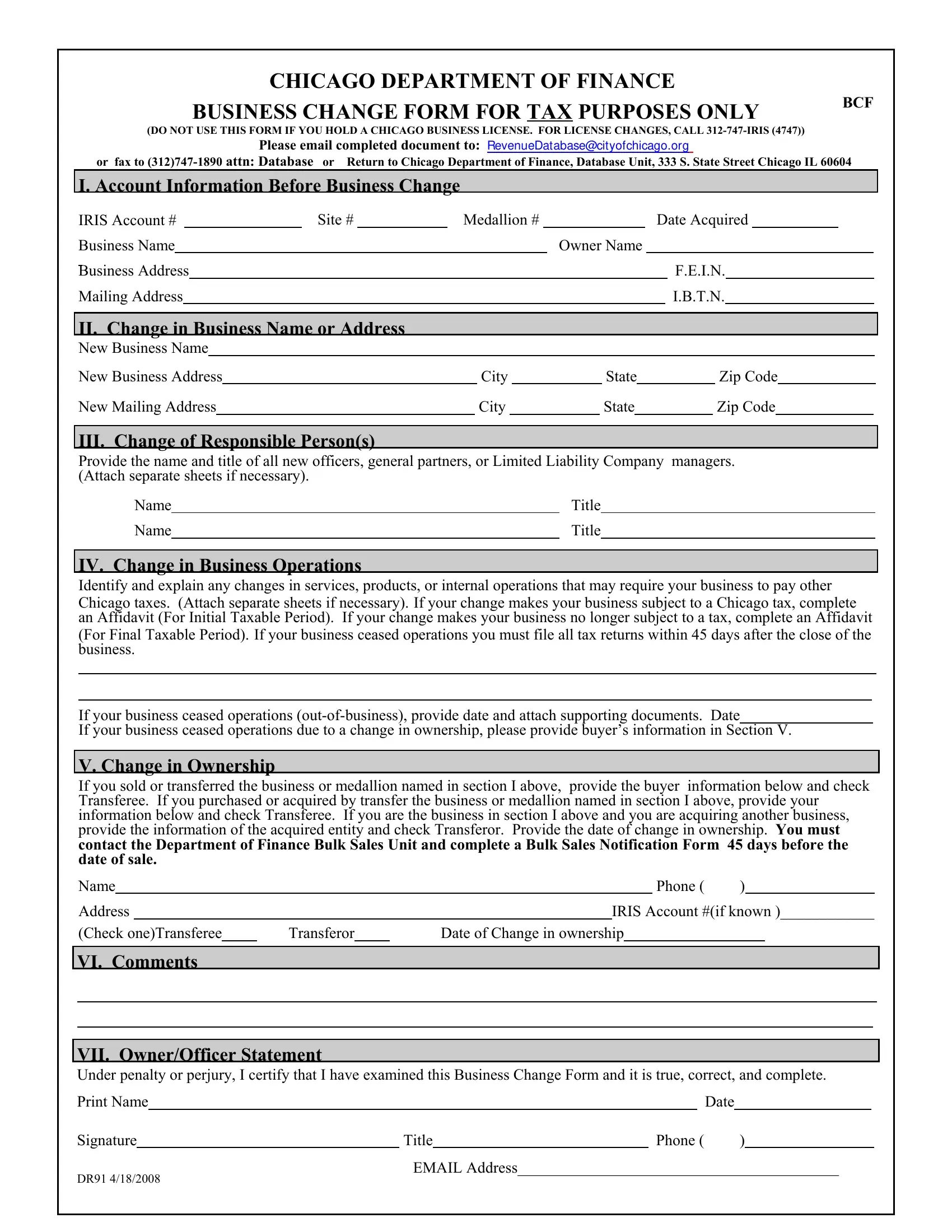
Navigating the complexities of business transitions in Chicago involves an array of procedures, with the Dr91 Chicago form standing as a pivotal document for those undergoing change. This form, designated by the Chicago Department of Finance and aimed solely at tax-related amendments, serves businesses that don't require alterations to their existing Chicago business licenses. Essential for ensuring compliance, the document facilitates updates ranging from ownership changes, adjustments in business operations, to modifications in business or mailing addresses, thereby requiring detailed account information from the outset. It demands accuracy in conveying new business details, shifts in responsible personnel, and any operational shifts that might affect tax liabilities. Additionally, it plays a crucial role in the process of business sales or transfers, incorporating sections for both parties involved. Completing and submitting this form not only aligns with legal stipulations but also ensures the continuity of operations without fiscal interruptions. The ease of submission, with options to email, fax, or mail, underscores the city's commitment to accommodating business needs amidst transitions, emphasizing the importance of timely and precise compliance to prevent potential complications.
| Question | Answer |
|---|---|
| Form Name | Form Dr91 Chicago |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | BusinessChangeF orm_3 city of chicago business change form |
CHICAGO DEPARTMENT OF FINANCE
BUSINESS CHANGE FORM FOR TAX PURPOSES ONLY
BCF
(DO NOT USE THIS FORM IF YOU HOLD A CHICAGO BUSINESS LICENSE. FOR LICENSE CHANGES, CALL
Please email completed document to: RevenueDat abase@cit yofchicago.org
or fax to |
or Return to Chicago Department of FINANCE, Database Unit, 333 S. State Street Chicago IL 60604 |
||||||||||||||||||||||||||||||
I. Account Information Before Business Change |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
IRIS Account # |
|
|
Site # |
|
|
Medallion # |
|
|
|
|
|
|
Date Acquired |
|
|
||||||||||||||||
Business Name |
|
|
|
|
|
|
|
|
|
|
Owner Name |
|
|
|
|
|
|
|
|
|
|
||||||||||
Business Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
F.E.I.N. |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Mailing Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I.B.T.N. |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
II. Change in Business Name or Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
New Business Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
New Business Address |
|
|
|
|
|
City |
|
|
|
State |
|
|
Zip Code |
||||||||||||||||||
New Mailing Address |
|
|
|
|
|
|
City |
|
|
|
|
State |
|
|
|
Zip Code |
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
III. Change of Responsible Person(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
Provide the name and title of all new officers, general partners, or Limited Liability Company |
managers. |
||||||||||||||||||||||||||||||
(Attach separate sheets if necessary). |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Name |
|
|
|
|
|
|
|
|
|
|
|
Title |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Name |
|
|
|
|
|
|
|
|
|
|
|
Title |
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
IV. Change in Business Operations
Identify and explain any changes in services, products, or internal operations that may require your business to pay other
Chicago taxes. (Attach separate sheets if necessary). If your change makes your business subject to a Chicago tax, complete an Affidavit (For Initial Taxable Period). If your change makes your business no longer subject to a tax, complete an Affidavit
(For Final Taxable Period). If your business ceased operations you must file all tax returns within 45 days after the close of the business.
If your business ceased operations
If your business ceased operations due to a change in ownership, please provide buyer’s information in Section V.
V. Change in Ownership
If you sold or transferred the business or medallion named in section I above, provide the buyer information below and check Transferee. If you purchased or acquired by transfer the business or medallion named in section I above, provide your information below and check Transferee. If you are the business in section I above and you are acquiring another business, provide the information of the acquired entity and check Transferor. Provide the date of change in ownership. You must contact the Department of FINANCE Bulk Sales Unit and complete a Bulk Sales Notification Form 45 days before the date of sale.
Name |
|
|
|
|
|
|
|
Phone ( |
) |
|
|
|
Address |
|
|
|
|
|
IRIS Account #(if known )____________ |
||||||
(Check one)Transferee |
|
Transferor |
|
Date of Change in ownership |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
VI. Comments
VII. Owner/Officer Statement
Under penalty or perjury, I certify that I have examined this Business Change Form and it is true, correct, and complete.
Print Name |
|
|
|
|
Date |
|
||||
|
|
|
|
|
|
|
|
|
|
|
Signature |
|
|
Title |
Phone ( |
) |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
EMAIL Address_________________________________________
DR91 4/18/2008