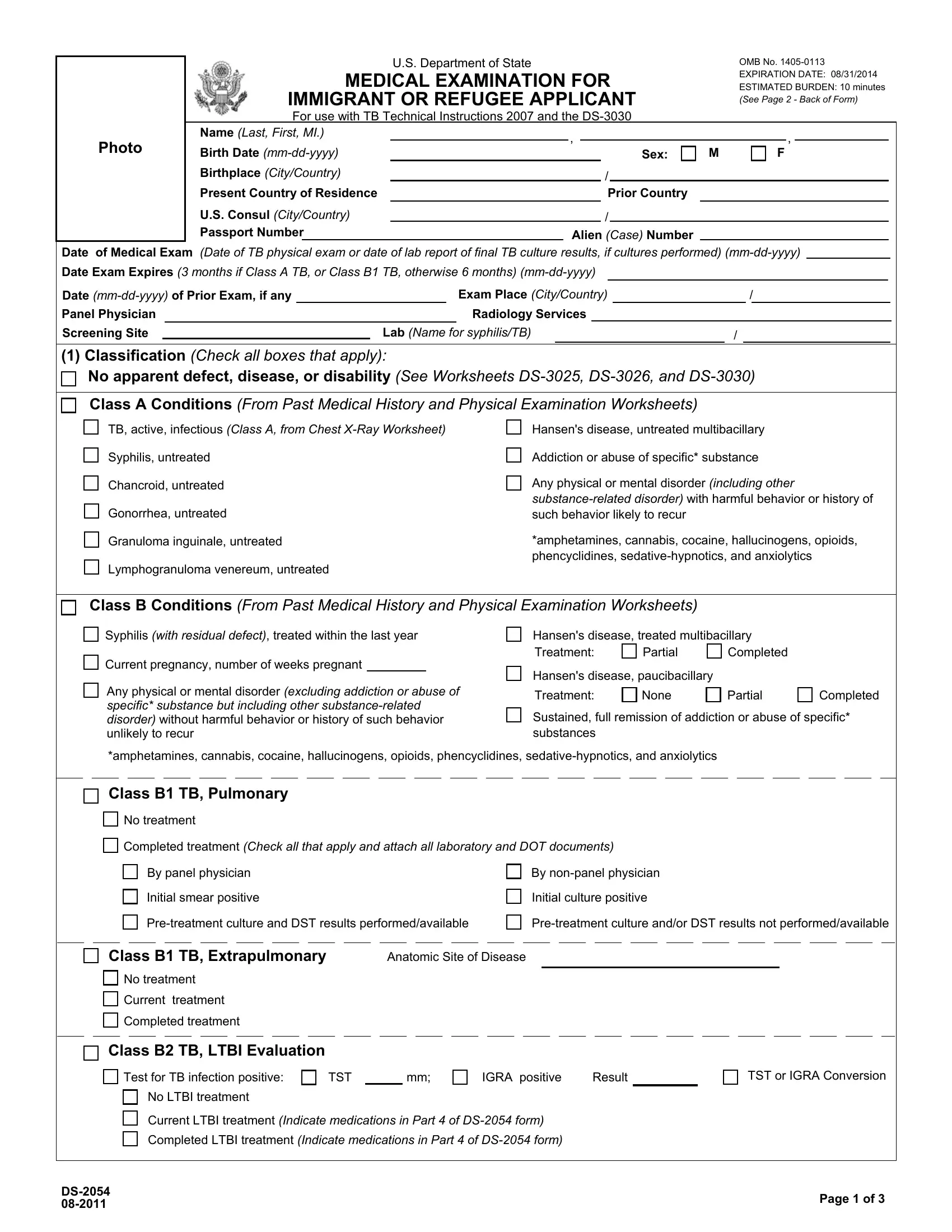
Embarking on the journey to becoming a lawful immigrant or refugee in the United States entails a thorough process, including the submission of the DS form, an integral document facilitated by the U.S. Department of State. It serves as a comprehensive medical examination form that must be completed by immigrant or refugee applicants, aligning with the TB Technical Instructions 2007 and the DS-3030. This document meticulously records personal information such as name, date of birth, and country of birth, alongside detailed medical examination results ranging from tuberculosis (TB) classifications to various infectious diseases assessments. Within its scope, the form categorizes medical conditions into Class A and Class B, distinguishing between more serious health conditions that could signify a public health risk and less severe issues. Additionally, the form addresses treatment histories, laboratory findings, and immunization records, ensuring that applicants meet the health standards required for entry into the U.S. It emphasizes the importance of transparency and accuracy, with the estimated burden of completing the form being around 10 minutes, although the impact on the applicant's journey is far more significant. By fulfilling the requirements outlined in the DS form, applicants take a crucial step toward their goal of residing in the United States, underpinning the process with a detail-oriented approach that underscores the intersection of public health and immigration policy.
| Question | Answer |
|---|---|
| Form Name | Form Ds 2054 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | ds2054 form ds 2054 |
