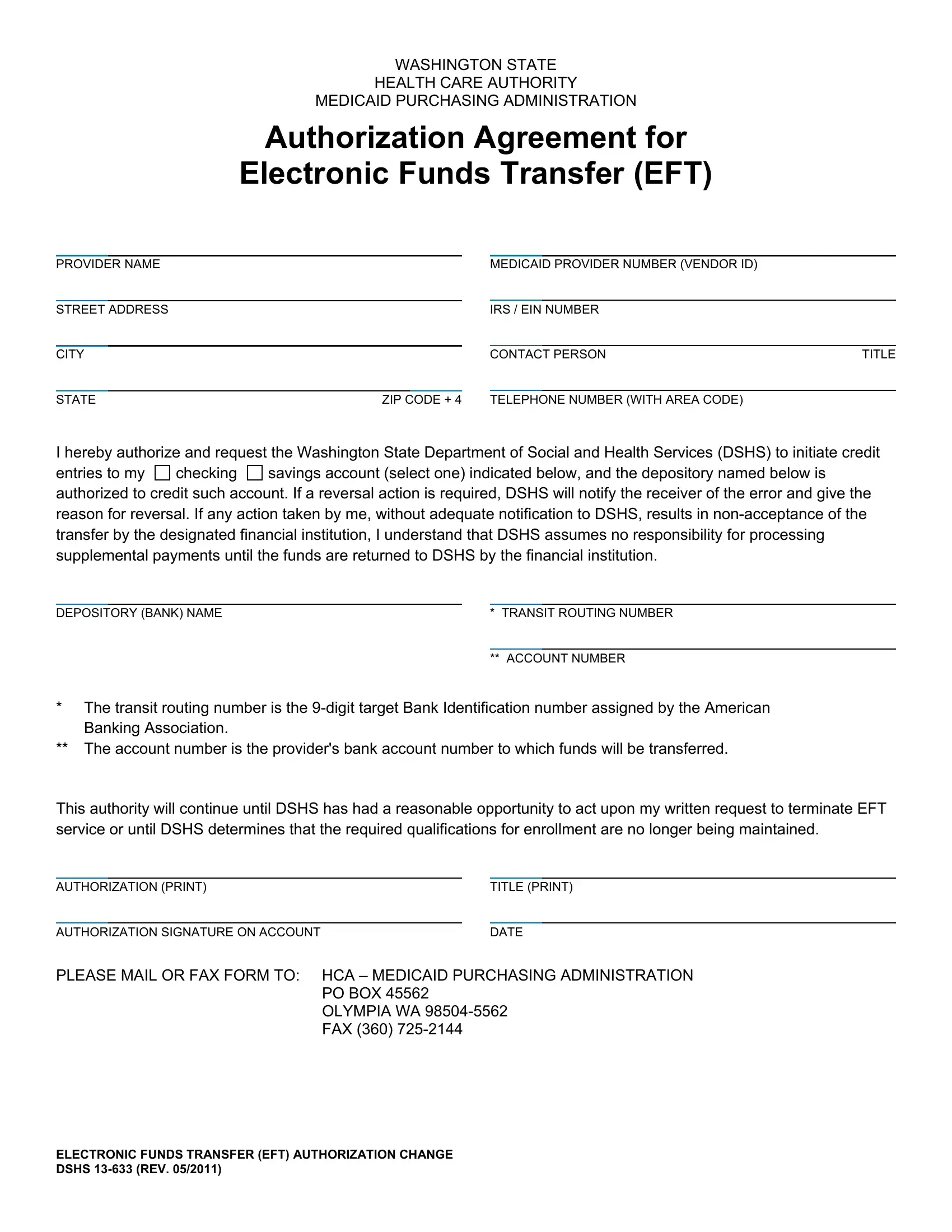
Navigating the process of receiving payments from Washington State's Department of Social and Health Services (DSHS) can be streamlined through the Authorization Agreement for Electronic Funds Transfer (EFT), documented in form DSHS 13-633. This critical form allows healthcare providers to receive Medicaid payments directly to their bank accounts, either checking or savings, ensuring a more efficient and secure transfer of funds. By completing this form, providers supply essential information including their provider name, Medicaid provider number (vendor ID), and address, alongside IRS or EIN numbers, ensuring the state can correctly identify and process payments. The form further requires bank details such as the depository name, transit routing number, and account number, setting a clear path for the funds. Authorization from the provider is mandated to initiate this process, incorporating a section for the account holder’s signature, title, and contact details, thus facilitating verification and communication. Importantly, this form signifies a provider's consent for DSHS to credit their account while establishing the provider's understanding that any actions leading to the non-acceptance of the transfer absolve DSHS of responsibility for issuing payments until the issue is resolved. The form also outlines conditions for termination of the EFT service or modifications to the agreement, ensuring both parties are aware of the procedural aspects. Completion and submission instructions are clearly stated, guiding providers on how to send the completed form to the relevant authority, thereby simplifying the enrollment process for electronic payments.
| Question | Answer |
|---|---|
| Form Name | Form Dshs 13 633 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | 18_633 dshs ein number form |
WASHINGTON STATE
HEALTH CARE AUTHORITY
MEDICAID PURCHASING ADMINISTRATION
Authorization Agreement for
Electronic Funds Transfer (EFT)
PROVIDER NAME |
|
|
|
MEDICAID PROVIDER NUMBER (VENDOR ID) |
|
||
|
|
|
|
|
|
|
|
STREET ADDRESS |
|
|
IRS / EIN NUMBER |
|
|||
|
|
|
|
|
|
|
|
CITY |
|
|
CONTACT PERSON |
TITLE |
|||
|
|
|
|
|
|
|
|
STATE |
ZIP CODE + 4 |
|
TELEPHONE NUMBER (WITH AREA CODE) |
|
|||
I hereby authorize and request the Washington State Department of Social and Health Services (DSHS) to initiate credit entries to my checking savings account (select one) indicated below, and the depository named below is authorized to credit such account. If a reversal action is required, DSHS will notify the receiver of the error and give the reason for reversal. If any action taken by me, without adequate notification to DSHS, results in
DEPOSITORY (BANK) NAME |
* TRANSIT ROUTING NUMBER |
|
|
|
|
|
** ACCOUNT NUMBER |
|
*The transit routing number is the
**The account number is the provider's bank account number to which funds will be transferred.
This authority will continue until DSHS has had a reasonable opportunity to act upon my written request to terminate EFT service or until DSHS determines that the required qualifications for enrollment are no longer being maintained.
AUTHORIZATION (PRINT) |
|
TITLE (PRINT) |
||
|
|
|
|
|
AUTHORIZATION SIGNATURE ON ACCOUNT |
|
DATE |
||
PLEASE MAIL OR FAX FORM TO: HCA – MEDICAID PURCHASING ADMINISTRATION
PO BOX 45562 OLYMPIA WA
ELECTRONIC FUNDS TRANSFER (EFT) AUTHORIZATION CHANGE DSHS