On November 1, 2017, the Department of Social and Health Services (DSHS) released Form Dshs 13 680 to all healthcare providers in Washington State. This new form is required for all medical practitioners who provide services covered by Apple Health (Medicaid), including dental and vision services. The form must be completed by the healthcare provider and submitted to DSHS within 30 days of providing service. Penalties may be assessed for noncompliance. Read on for more information about this new form and what it means for healthcare providers in Washington State.
| Question | Answer |
|---|---|
| Form Name | Form Dshs 13 680 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 13_680 dshs bh forms |
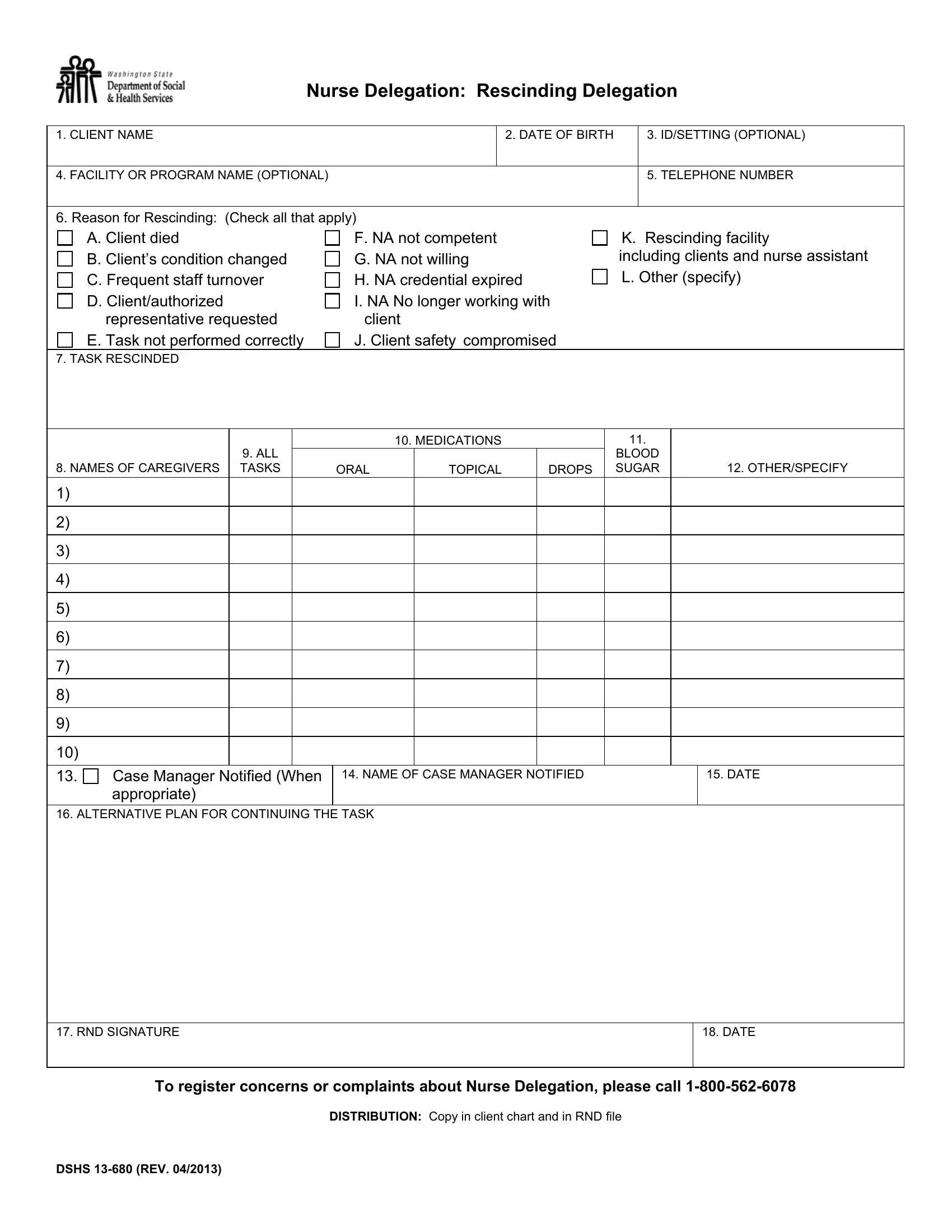
Nurse Delegation: Rescinding Delegation
1. CLIENT NAME |
|
|
|
|
|
2. DATE OF BIRTH |
|
3. ID/SETTING (OPTIONAL) |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. FACILITY OR PROGRAM NAME (OPTIONAL) |
|
|
|
|
|
|
|
|
|
5. TELEPHONE NUMBER |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
6. Reason for Rescinding: (Check all that apply) |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
A. Client died |
|
F. NA not competent |
|
|
|
K. Rescinding facility |
|||||||||
|
B. Client’s condition changed |
|
G. NA not willing |
|
|
|
including clients and nurse assistant |
|||||||||
|
C. Frequent staff turnover |
|
H. NA credential expired |
L. Other (specify) |
||||||||||||
|
D. Client/authorized |
|
I. NA No longer working with |
|
|
|
|
|
||||||||
|
representative requested |
|
client |
|
|
|
|
|
|
|
|
|||||
|
E. Task not performed correctly |
|
J. Client safety compromised |
|
|
|
|
|
||||||||
7. TASK RESCINDED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
10. MEDICATIONS |
|
|
|
11. |
|
|
|
|||
|
|
9. ALL |
|
|
|
|
|
|
|
|
|
BLOOD |
|
|
|
|
8. NAMES OF CAREGIVERS |
TASKS |
|
|
ORAL |
|
TOPICAL |
|
DROPS |
|
SUGAR |
|
|
12. OTHER/SPECIFY |
|||
1) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
13. |
Case Manager Notified (When |
|
14. NAME OF CASE MANAGER NOTIFIED |
|
|
|
|
15. DATE |
||||||||
|
appropriate) |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
16. ALTERNATIVE PLAN FOR CONTINUING THE TASK |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
17. RND SIGNATURE |
|
|
|
|
|
|
|
|
|
|
|
|
18. DATE |
|||
|
|
|
||||||||||||||
|
To register concerns or complaints about Nurse Delegation, please call |
|||||||||||||||
|
|
|
|
DISTRIBUTION: Copy in client chart and in RND file |
|
|
|
|||||||||
DSHS
Instructions for Completing Nurse Delegation: Rescinding Delegation
All fields are required unless indicated “OPTIONAL”.
1.Client Name: Enter ND client’s name (last name, first name).
2.Date of Birth: Enter ND client’s date of birth (month, day, year).
3.ID Setting: OPTIONAL – Enter client’s ID number as assigned by your business OR enter settings “AFH”, “ALF”,
DDDProgram,
4.Facility or Program Name: OPTIONAL – Enter name of facility/program contact.
5.Telephone Number: OPTIONAL – Enter telephone number of facility/program contact including area code.
6.Reason for Rescinding: Mark the boxes next to the reason for rescinding. Mark all that apply.
7.Task Rescinded: Enter name of task rescinded. If medication, list name. This applies to all caregivers delegated for this task.
8.Names of Caregivers: Enter name of individual caregiver rescinded. If all, enter “ALL”.
9.All Tasks: Enter “X” under all tasks next to name of appropriate caregiver(s).
10.Medications: Enter name of individual medication if appropriate. If all, enter “ALL”.
11.Blood Sugar: Enter “X” if blood sugar rescinded.
12.Other/Specify: OPTIONAL – List other tasks rescinded or list date if appropriate.
13.OPTIONAL – Check the box if appropriate. Case Manager must be notified if ALL tasks (client condition has changed) are rescinded or ALL caregivers (client unable to receive needed services).
14.Name of Case Manager Notified: Enter case manager name, if notified.
15.Date: Enter date the case manager was notified.
16.Alternative Plan for Continuing the Task: Describe how client’s needs will continue to be met.
17.and 18. RND Signature and Date: Sign and date your signature. The date the form is signed is the date of rescinding, unless otherwise noted in #7.
DSHS