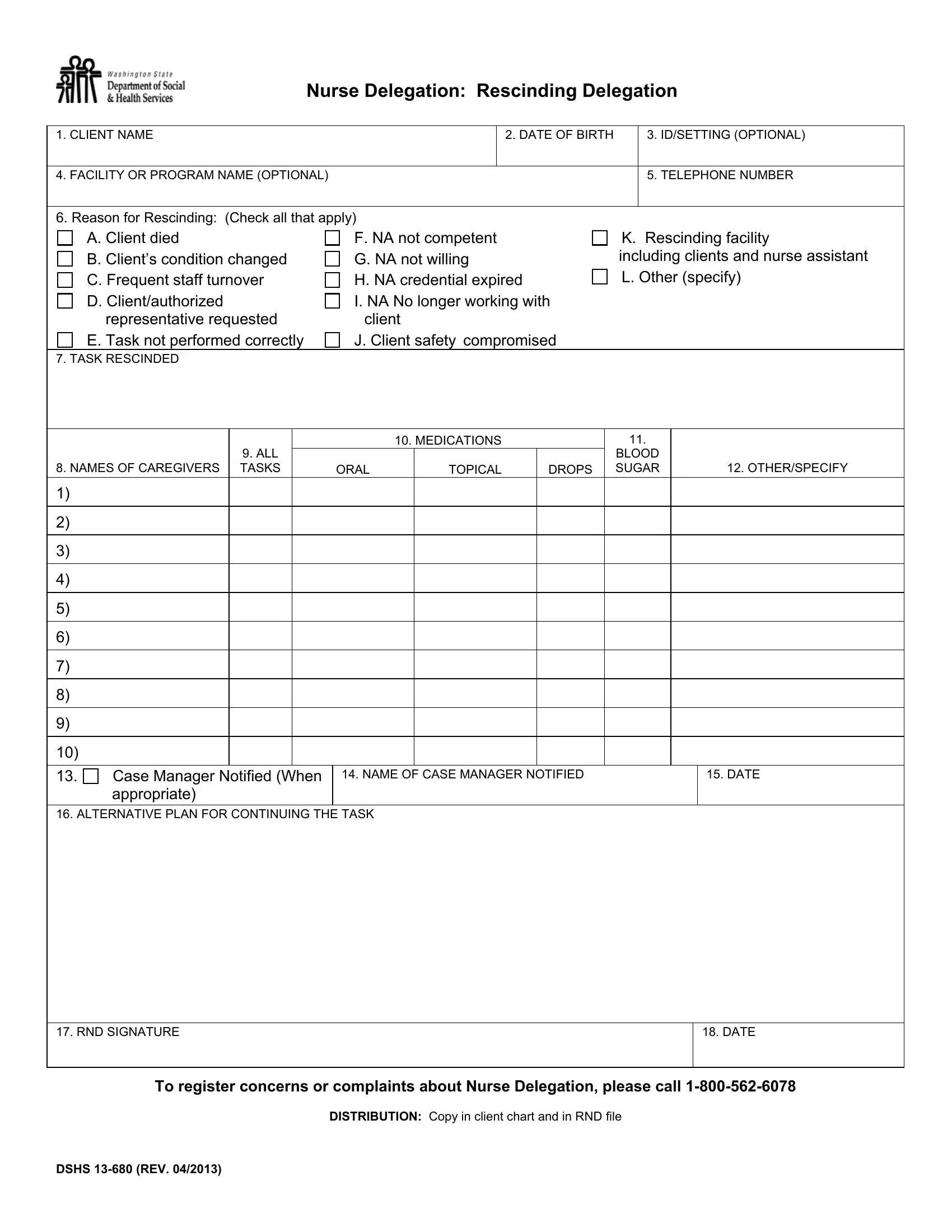
The DSHS 13-680 form plays a crucial role in the nurse delegation process, particularly when it becomes necessary to rescind a previously delegated nursing task. This procedural action can be initiated for a variety of reasons, as indicated on the form, which includes situations such as the death of a client, significant changes in a client's condition, issues related to the competency or willingness of a nursing assistant (NA), among others. The form meticulously outlines the process for formally rescinding delegation, requiring detailed entries including client information, specific tasks being rescinded, names of caregivers affected, and instructions for mediations, if applicable. Notably, it prioritizes client safety and continuity of care by requiring notification of a case manager when appropriate and the formulation of an alternative plan to ensure the client's needs are met post-rescission. With fields for signatures and dates, the form serves as an official record of the decision to withdraw a delegated task, ensuring accountability and providing a clear framework for adapting to changes in a client's care requirements. This document, revised in April 2013, insists on a structured communication between nursing professionals and administrative bodies, thereby upholding the standards of nursing care and client safety.
| Question | Answer |
|---|---|
| Form Name | Form Dshs 13 680 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 13_680 dshs bh forms |
Nurse Delegation: Rescinding Delegation
1. CLIENT NAME |
|
|
|
|
|
2. DATE OF BIRTH |
|
3. ID/SETTING (OPTIONAL) |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. FACILITY OR PROGRAM NAME (OPTIONAL) |
|
|
|
|
|
|
|
|
|
5. TELEPHONE NUMBER |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
6. Reason for Rescinding: (Check all that apply) |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
A. Client died |
|
F. NA not competent |
|
|
|
K. Rescinding facility |
|||||||||
|
B. Client’s condition changed |
|
G. NA not willing |
|
|
|
including clients and nurse assistant |
|||||||||
|
C. Frequent staff turnover |
|
H. NA credential expired |
L. Other (specify) |
||||||||||||
|
D. Client/authorized |
|
I. NA No longer working with |
|
|
|
|
|
||||||||
|
representative requested |
|
client |
|
|
|
|
|
|
|
|
|||||
|
E. Task not performed correctly |
|
J. Client safety compromised |
|
|
|
|
|
||||||||
7. TASK RESCINDED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
10. MEDICATIONS |
|
|
|
11. |
|
|
|
|||
|
|
9. ALL |
|
|
|
|
|
|
|
|
|
BLOOD |
|
|
|
|
8. NAMES OF CAREGIVERS |
TASKS |
|
|
ORAL |
|
TOPICAL |
|
DROPS |
|
SUGAR |
|
|
12. OTHER/SPECIFY |
|||
1) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
13. |
Case Manager Notified (When |
|
14. NAME OF CASE MANAGER NOTIFIED |
|
|
|
|
15. DATE |
||||||||
|
appropriate) |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
16. ALTERNATIVE PLAN FOR CONTINUING THE TASK |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
17. RND SIGNATURE |
|
|
|
|
|
|
|
|
|
|
|
|
18. DATE |
|||
|
|
|
||||||||||||||
|
To register concerns or complaints about Nurse Delegation, please call |
|||||||||||||||
|
|
|
|
DISTRIBUTION: Copy in client chart and in RND file |
|
|
|
|||||||||
DSHS
Instructions for Completing Nurse Delegation: Rescinding Delegation
All fields are required unless indicated “OPTIONAL”.
1.Client Name: Enter ND client’s name (last name, first name).
2.Date of Birth: Enter ND client’s date of birth (month, day, year).
3.ID Setting: OPTIONAL – Enter client’s ID number as assigned by your business OR enter settings “AFH”, “ALF”,
DDDProgram,
4.Facility or Program Name: OPTIONAL – Enter name of facility/program contact.
5.Telephone Number: OPTIONAL – Enter telephone number of facility/program contact including area code.
6.Reason for Rescinding: Mark the boxes next to the reason for rescinding. Mark all that apply.
7.Task Rescinded: Enter name of task rescinded. If medication, list name. This applies to all caregivers delegated for this task.
8.Names of Caregivers: Enter name of individual caregiver rescinded. If all, enter “ALL”.
9.All Tasks: Enter “X” under all tasks next to name of appropriate caregiver(s).
10.Medications: Enter name of individual medication if appropriate. If all, enter “ALL”.
11.Blood Sugar: Enter “X” if blood sugar rescinded.
12.Other/Specify: OPTIONAL – List other tasks rescinded or list date if appropriate.
13.OPTIONAL – Check the box if appropriate. Case Manager must be notified if ALL tasks (client condition has changed) are rescinded or ALL caregivers (client unable to receive needed services).
14.Name of Case Manager Notified: Enter case manager name, if notified.
15.Date: Enter date the case manager was notified.
16.Alternative Plan for Continuing the Task: Describe how client’s needs will continue to be met.
17.and 18. RND Signature and Date: Sign and date your signature. The date the form is signed is the date of rescinding, unless otherwise noted in #7.
DSHS