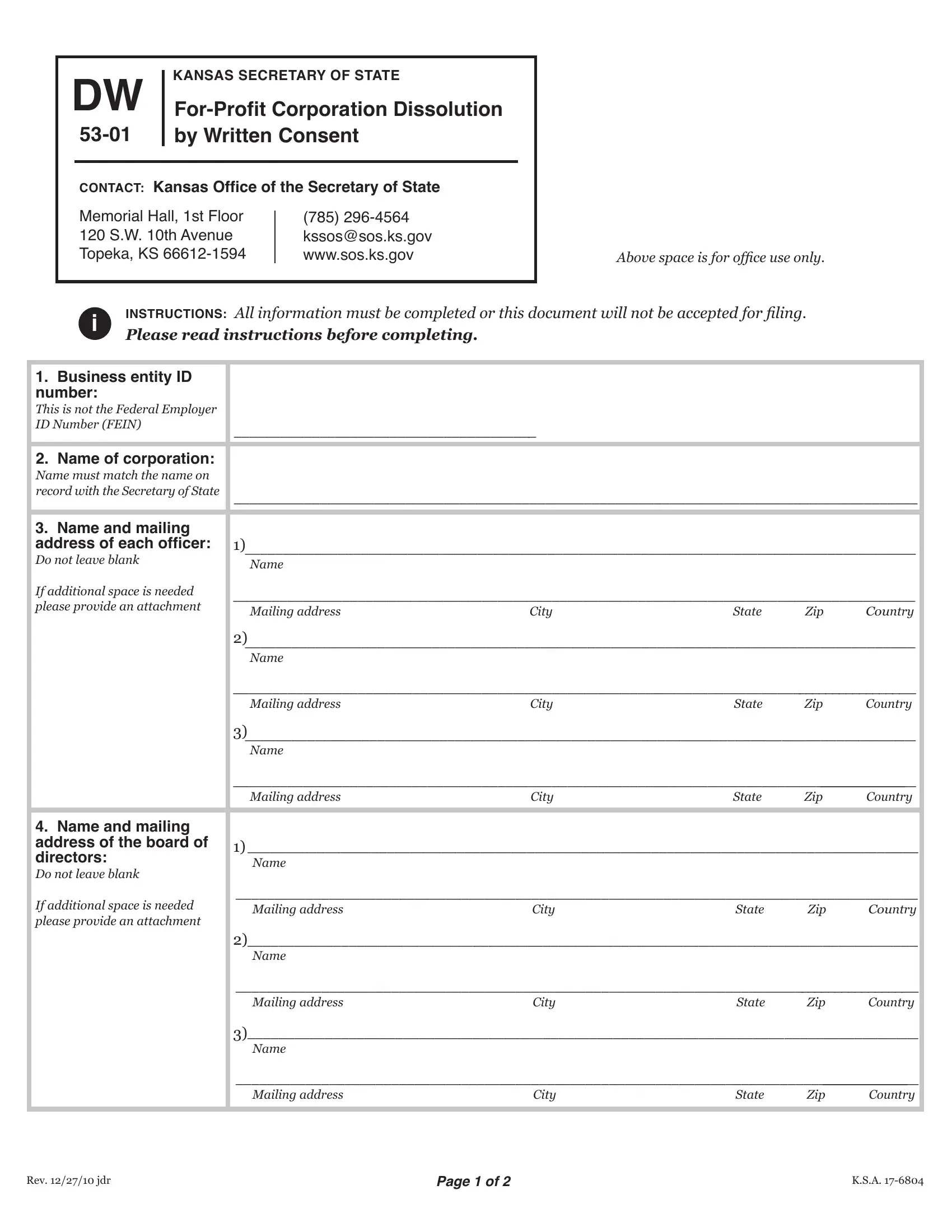
When a for-profit corporation based in Kansas decides to cease its operations, a crucial step in the process involves the submission of the DW 53-01 form to the Kansas Secretary of State. This form, officially titled "For-Profit Corporation Dissolution by Written Consent," serves as a formal declaration of the company's intent to dissolve. The form requires comprehensive details about the corporation, including its business entity ID number, the official name as recorded by the Secretary of State, and the names and addresses of its officers and board of directors. A key aspect of this form is the unanimous consent for dissolution from all stockholders with voting power, a testament to the collective agreement on this significant decision. It also outlines the requirement that the effective date of dissolution be mentioned, which can be immediate upon filing or scheduled for a specific date within 90 days of the filing. Furthermore, the form includes a declaration made under penalty of perjury by an officer of the corporation, affirming the truthfulness of the information provided and confirming that all necessary stockholder consents have been obtained. Alongside the filled form, a filing fee is required, emphasizing the formal nature of this process. Entities are also reminded of certain prerequisites such as settling annual reports and fees, and if needed, reinstating the corporation before dissolution. The form, complemented by clear instructions and additional notes, underscores the importance of accurate completion and timely submission to ensure a smooth dissolution process tailored to the legal framework set by Kansas state laws.
| Question | Answer |
|---|---|
| Form Name | Form Dw 53 01 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | DW instructions for dw 53 01 form |

|
DW |
|
KANSAS SECRETARY OF STATE |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
||||||||
|
|
by Written Consent |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|||||||
|
|
CONTACT: Kansas Ofice of the Secretary of State |
|
|
|
|
|
|||||||
|
|
Memorial Hall, 1st Floor |
|
|
|
|
|
|
||||||
|
|
(785) |
|
|
|
|
|
|||||||
|
|
120 S.W. 10th Avenue |
|
|
kssos@sos.ks.gov |
|
|
|
|
|
||||
|
|
Topeka, KS |
|
www.sos.ks.gov |
|
|
Above space is for ofice use only. |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
i |
INSTRUCTIONS: All information must be completed or this document will not be accepted for iling. |
|
||||||||||
|
|
Please read instructions before completing. |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
1. Business entity ID |
|
|
|
|
|
|
|
|
|
|||||
number: |
|
|
|
|
|
|
|
|
|
|
|
|
||
This is not the Federal Employer |
|
|
|
|
|
|
|
|
|
|||||
ID Number (FEIN) |
|
|
|
_______________________________________ |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
2. Name of corporation: |
|
|
|
|
|
|
|
|
|
|||||
Name must match the name on |
|
|
|
|
|
|
|
|
|
|||||
record with the Secretary of State |
|
________________________________________________________________________________________ |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||
3. Name and mailing |
|
|
|
|
|
|
|
|
|
|||||
address of each oficer: |
|
1)______________________________________________________________________________________ |
||||||||||||
Do not leave blank |
|
|
|
|
Name |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
If additional space is needed |
|
_______________________________________________________________________________________ |
||||||||||||
please provide an attachment |
|
|
Mailing address |
City |
State |
Zip |
Country |
|||||||
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
2)______________________________________________________________________________________ |
|||||||
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
__________________________________________________________________________________________ |
|||||||
|
|
|
|
|
|
|
|
Mailing address |
City |
State |
Zip |
Country |
||
|
|
|
|
|
|
|
3)_____________________________________________________________________________________ |
|||||||
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
____________________________________________________________________________________________________ |
|||||||
|
|
|
|
|
|
|
|
Mailing address |
City |
State |
Zip |
Country |
||
|
|
|
|
|
|
|
|
|
|
|||||
4. Name and mailing |
|
|
|
|
|
|
|
|
|
|||||
address of the board of |
|
1)______________________________________________________________________________________ |
||||||||||||
directors: |
|
|
|
|
|
Name |
|
|
|
|
|
|||
Do not leave blank |
|
|
|
|
|
|
|
|
|
|
|
|||
If additional space is needed |
|
_______________________________________________________________________________________ |
||||||||||||
|
|
Mailing address |
City |
State |
Zip |
Country |
||||||||
please provide an attachment |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
2)______________________________________________________________________________________ |
|||||||
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
__________________________________________________________________________________________ |
|||||||
|
|
|
|
|
|
|
|
Mailing address |
City |
State |
Zip |
Country |
||
|
|
|
|
|
|
|
3) |
_____________________________________________________________________________________ |
||||||
|
|
|
|
|
|
|
Name |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
____________________________________________________________________________________________________ |
|||||||
|
|
|
|
|
|
|
|
Mailing address |
City |
State |
Zip |
Country |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Rev. 12/27/10 jdr |
Page 1 of 2 |
K.S.A. |
5.All stockholders with voting power do hereby consent to the dissolution of the corporation: Stockholders’ signatures
____________________________________________ |
_______________________________________________ |
|||
____________________________________________ |
_______________________________________________ |
|||
____________________________________________ |
_______________________________________________ |
|||
____________________________________________ |
_______________________________________________ |
|||
____________________________________________ |
_______________________________________________ |
|||
|
|
|
|
|
6. Effective date: |
|
Upon iling |
|
|
A future effective date must be |
|
|
|
|
within 90 days of iling date |
|
Future effective date ______________________________ |
||
|
|
|||
|
|
Month |
Day |
Year |
|
|
|
|
|
7. I, _______________________________________, declare under penalty of perjury under the laws of the state of |
||||
Name of oficer |
|
|
||
Kansas, that I am an oficer of the |
||||
of ALL stockholders entitled to vote on the dissolution, that the foregoing is true and correct and that I have remitted |
||||
the required fee. |
|
|
|
|
________________________________________________________ |
________________________________________________________ |
|||
Signature of secretary or other oficer |
Date (month, day, year) |
|||
________________________________________________________ |
|
|
||
Name of signer (printed or typed) |
|
|
|
|
iInstructions:
1. If this form is submitted after the close of the entity’s tax year, an annual report and fee must be iled along with or
prior to dissolution. If the entity has forfeited, it must reinstate before dissolution.
2. Submit this form with the $35 filing fee.
STAY
NOTICE: There is a $25 service fee for all checks returned by your inancial institution.
All information must be completed or this document will not be accepted for iling.
Rev. 12/27/10 jdr |
Page 2 of 2 |
K.S.A. |